4922
Early enhancement heterogeneity and density on ultrafast bilateral DCE-MRI may differentiate benign and malignant breast lesionsFederico Pineda1, Naoko Mori2, Hiroyuki Abe1, David Schacht1, and Gregory Karczmar1
1Radiology, University of Chicago, Chicago, IL, United States, 2Tohoku University
Synopsis
Heterogeneity of enhancement has been shown to be a marker for malignancy in breast DCE-MRI, however standard dynamic protocols typically have low temporal resolution (60 to 90 seconds). Fast protocols have the advantage of accurately measuring early lesion kinetics. Heterogeneity of lesion enhancement in the first time-point (6 to 9 seconds) after arterial enhancement in the breast differed significantly between malignant and benign lesions; differences were not significant at later time-points.
Purpose
Enhancement heterogeneity has been used previously to identify breast tumors on DCE-MRI methods1. However, this previous work was based on low temporal resolution imaging that did not capture the kinetics of enhancement heterogeneity at early times after contrast media injection. Here we evaluated diagnostic utility of enhancement heterogeneity at early times post-injection in ultrafast bilateral DCE-MR images acquired with temporal resolution of 6-9 seconds per image.Methods
20 women with enhancing lesions (18 malignant lesions and 17 benign) underwent breast DCE-MRI examinations using an 'ultrafast' protocol for the first minute post-contrast administration. Images were acquired on a 3T scanner using a 16-channel bilateral breast coil. Temporal resolution during the first minute post-contrast was 6 to 9 seconds per time-point, using standard Cartesian acquisition and reconstruction methods (and modestly reduced spatial resolution). Temporal resolution in standard clinical bilateral breast DCE-MRI protocols is typically 60 – 90 seconds. Initial experience with the ultrafast protocol showed that malignant lesions begin to enhance earlier and have higher early enhancement than benign lesions. Regions-of-interest (ROIs) were drawn on the final ultrafast acquisition and propagated to every time-point. Percent signal enhancement was calculated for each lesion voxel. Lesion heterogeneity was estimated using the median absolute deviation (MAD), a measure of how much the enhancement in each voxel differed from the median enhancement in the whole lesion. The density of enhancing voxels in each lesion was calculated by measuring the number of voxels that exceeded a threshold of 25% signal enhancement and dividing by the total number of voxels in the lesion. Measurements were performed on images after initial arterial enhancement in the breast, to account for inter-patient variability (e.g. cardiac output). Lesion classification performance was evaluated with ROC analysis.Results
Examples of benign and malignant lesions and signal enhancement color-maps can be seen in Figure 1. Lesion enhancement heterogeneity (measured with MAD) was significantly different between benign and malignant lesions (p < 0.05) at the first time-point after arterial enhancement. Density of signal enhancement was significantly different in benign vs. malignant lesions (p < 0.05) in the first three time-points after arterial enhancement. The malignant-to-benign ratio at the first time-point for MAD was 1.95 ± 0.75 and the ratio of enhancement density was 1.84 ± 0.90; these ratios decreased at later times. The area under the ROC curve (AUC) for MAD was 0.81 and 0.79 for enhancement density at the first time-point post arterial enhancement (Fig. 2).Discussion
Ultrafast imaging during the initial phase of enhancement provides the advantage of accurate measurements of early lesion kinetics, when the malignant-to-benign parameter ratios may be at their highest. These protocols also have the advantage of measuring kinetics relative to the bolus time-of-arrival, reducing variability due to global parameters. The very early phase of enhancement provides information that is not available from conventional MRI, and may be a useful aid for classifying breast lesions. Lesion enhancement heterogeneity and density could be added to conventional MRI parameters to increase overall diagnostic accuracy. Even higher temporal resolution may be useful, since with the current protocol, the malignant-to-benign ratios were highest at the first time-point after arterial enhancement. The performance of heterogeneity-related parameters will be more extensively evaluated in a larger cohort.Conclusion
The results suggest that certain early kinetic and morphological parameters can aid in lesion differentiation. In this study we found significant differences in lesion enhancement heterogeneity and enhancement density in the first 6 to 9 seconds after initial arterial enhancement in the breast.Acknowledgements
No acknowledgement found.References
1. Karahaliou A, Vassiou K, Arkidis NS, et al. Assessing heterogeneity of lesion enhancement kinetics in dynamic contrast-enhanced MRI for breast cancer diagnosis. Br J Radiol. 2010;83(988):296-309Figures
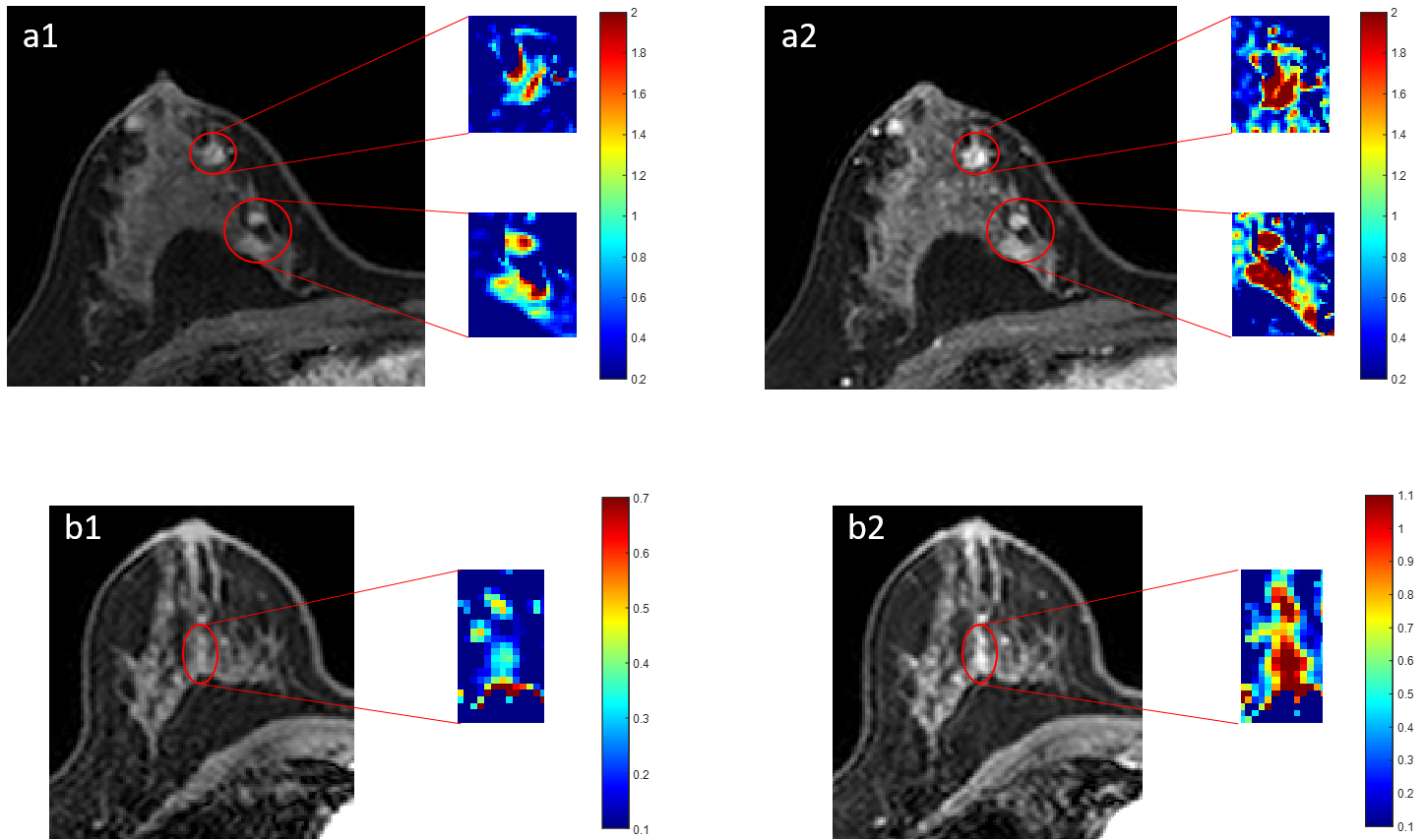
Example images from two cases, from the first time-point (~7s) after arterial enhancement in the breast (1) and ~30s later (2). (a) Invasive ductal carcinoma (IDC) masses. (b) Usual ductal hyperplasia. Color-maps indicate relative enhancement.
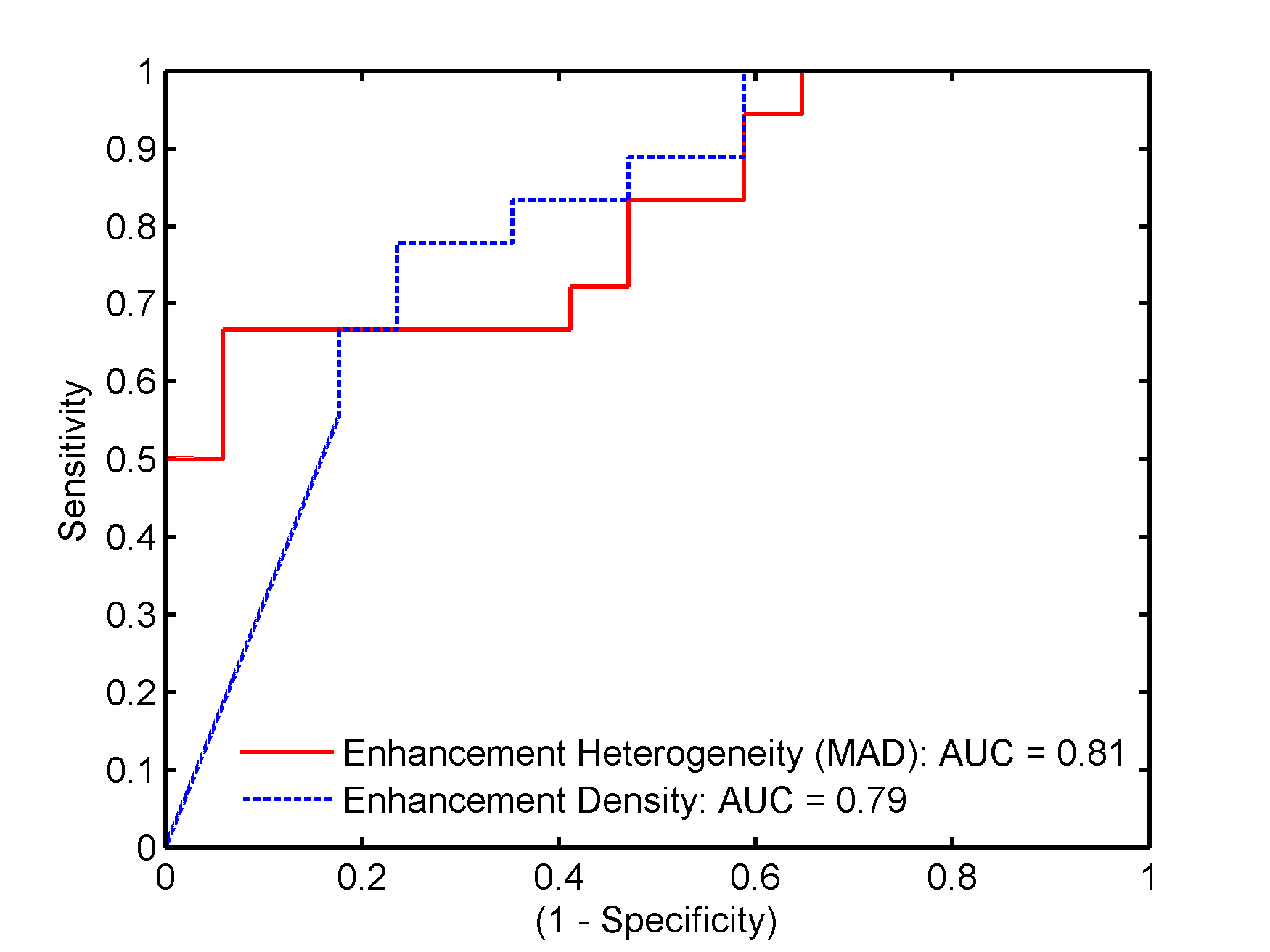
Receiver operating characteristic (ROC) curves for the use of enhancement density, and heterogeneity of enhancement (median absolute deviation) as lesion classifiers.