4920
Breast Cancer and Body Adiposity by Breast MRI1Division of Cancer Imaging Research, Department of Radiology, The Johns Hopkins University School of Medicine, BALTIMORE, MD, United States, 2Department of Oncology, The Sidney Kimmel Comprehensive Cancer Center, The Johns Hopkins University School of Medicine
Synopsis
Using the thickness of the upper abdominal adipose layer measured from breast MRI as a surrogate body adiposity marker, this retrospective investigation validated a positive correlation between breast cancer and body adiposity in a cohort of 1616 breast MRI patients. Additionally, triple negative breast cancer was significantly associated with a younger age and higher body adiposity with respect to the hormone receptor positive breast cancer, while the hormone and HER-2 receptor positive (triple positive) type is only associated with a younger age. A trend of low body adiposity was observed in DCIS patients in the 30 – 49 age range.
Introduction
Breast MRI is frequently used for breast cancer (BC) diagnosis, staging, and screening in population at elevated risk. We have utilized the thickness of the upper abdominal adipose layer (UAAL) measured from breast MRI exams as a surrogate body adiposity marker in previous studies due to the lack of body mass index (BMI) information 1, 2. This study is focused on the association between BC type, receptor status, age, and body adiposity. New correlation between the thickness of the UAAL and BMI is also reported.Methods
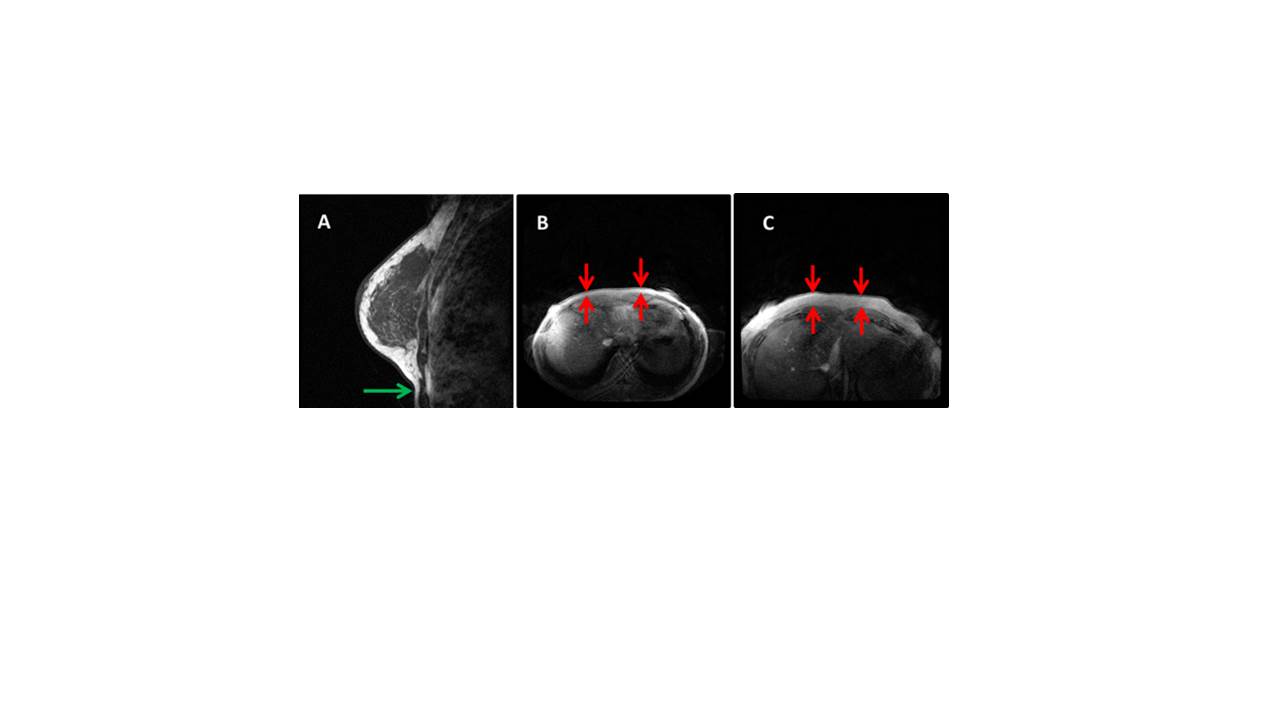
Breast MRI images acquired in our institution since 2008 were reviewed consecutively in the PACS in this IRB approved retrospective study. Corresponding patient electronic medical records were subsequently reviewed to confirm the presence or absence of a BC diagnosis. Relevant BC type and receptor status were retrieved from pathology reports. The thickness of the UAAL immediately below the breasts was measured on 3D axial T1 weighted breast MRI without fat saturation, Figure 1. This thickness was used as a surrogate body adiposity marker. BMI measured during a doctor’s visit within 6 month of the breast MRI was also retrieved from the medical records. Multinomial/multivariate logistic regression and Kruskal-Wallis test were performed in RStudio.Results
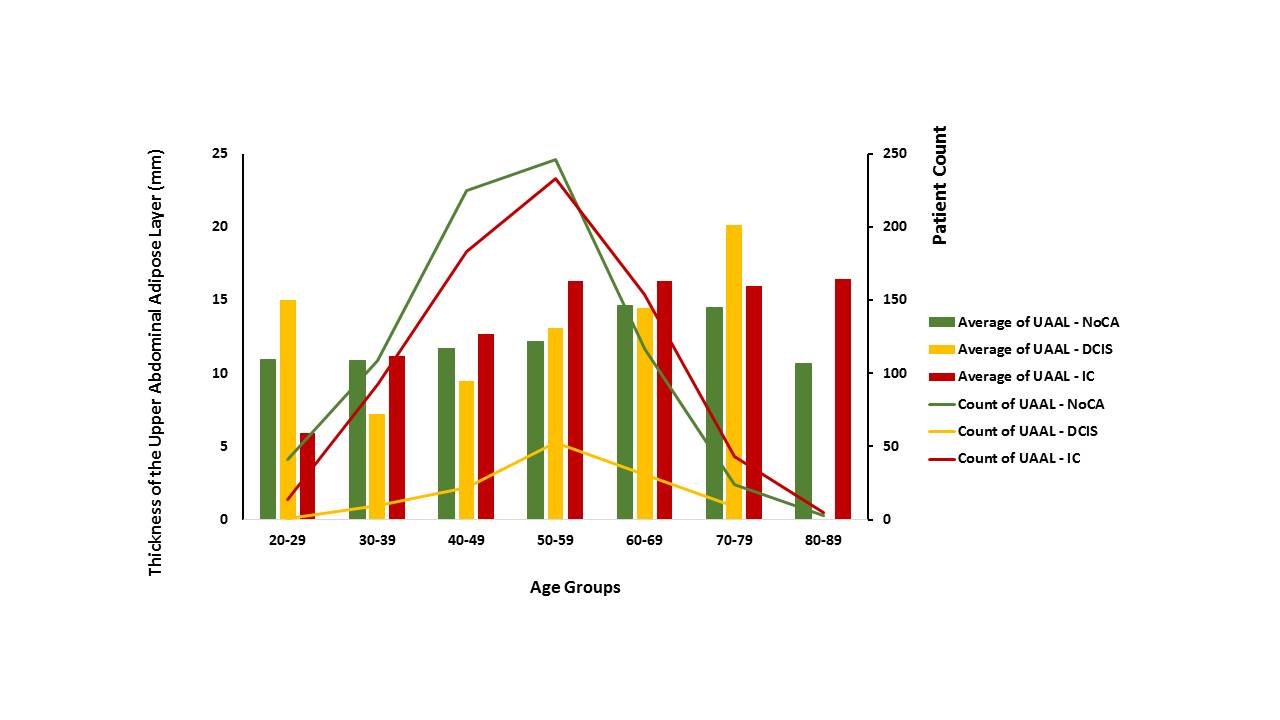
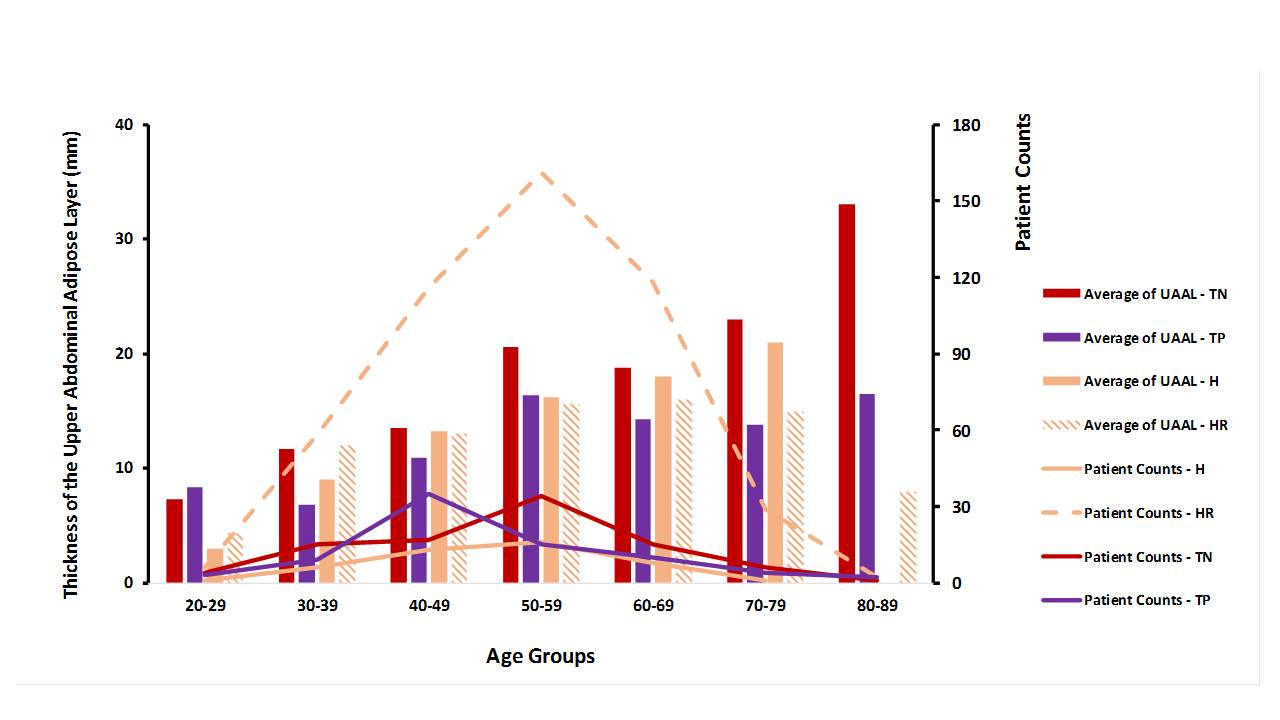
Breast cancer and body adiposity and age: A total of 1616 (724 invasive BC, 126 DCIS, and 766 benign findings) were identified from the breast MRI and medical database. Multinomial/multivariate logistic regression identified a significant association between BC and increased body adiposity and age (p < 0.001), using subjects without BC as a reference. The impact of body adiposity was most significant in the peak BC incidence age range of 50 – 59, Figure 2. Those diagnosed with DCIS had significantly lower body adiposity in the 40 – 49 age range (p < 0.05). Variation in body adiposity by BC receptor status was observed in some age groups, Figure 3. Multinomial/multivariate regression demonstrated a significant association between increased body adiposity and triple negative (TN) BC (p < 0.001), and a trend of negative association between body adiposity and hormone and HER-2 receptor positive (triple positive = TP) BC (p = 0.08), using subjects with hormone receptor positive (HR) BC as a reference. The mean age of TN, HR, HER-2 positive (H), and TP BC patients was 51.4, 53.1, 50.4, and 49.2, respectively. The occurrence of TP BC peaked in the 40 – 49 age range and all other subtypes of BC peaked in the 50 – 59 range, Figure 3.
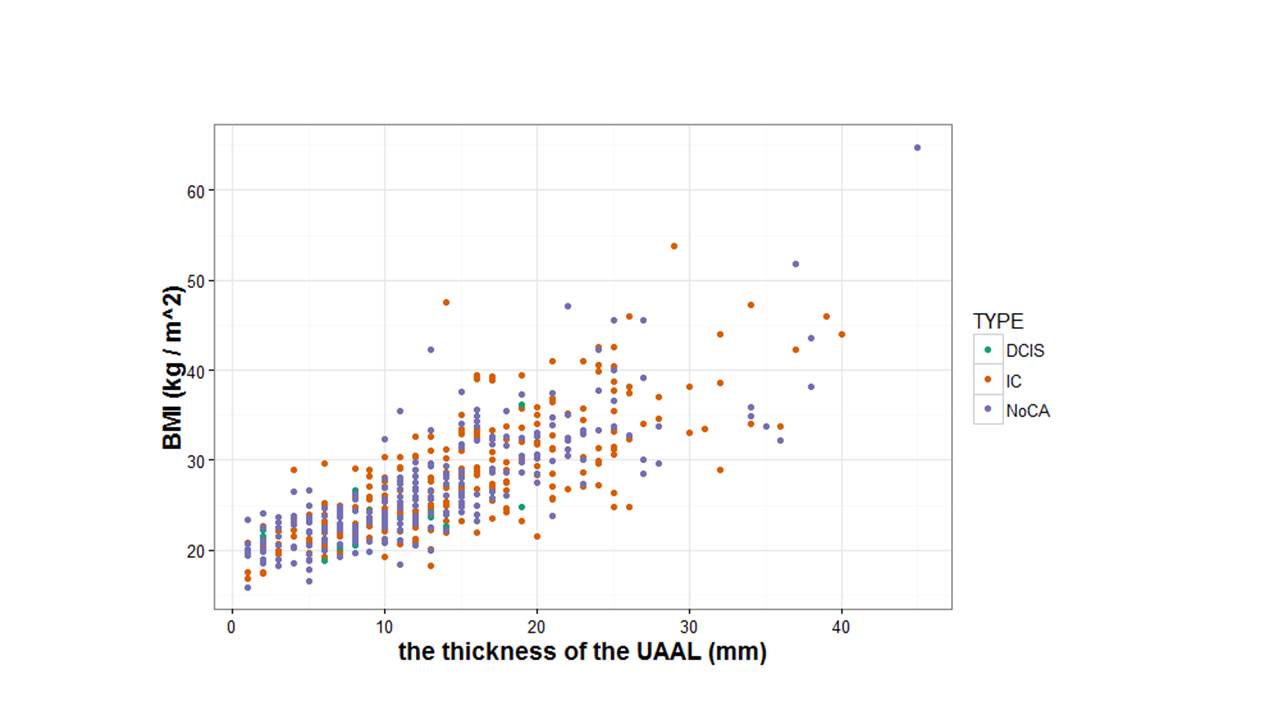
The correlation between the thickness of the UAAL and BMI: BMI has been measured during office visits and was incorporated into the medical records in recent years in our institution. The official BMI was available in 533 of the 1616 breast MRI patients. The nonparametric Spearman’s rank correlation coefficient between the thickness of the UAAL and BMI was 0.80 (p <0.001), Figure 4. A similar correlation pattern between the thickness of the UAAL and BMI was observed in patients without BC, with DCIS, and with invasive BC, Figure 4.
Discussion
Our results demonstrated a positive correlation between BC and body adiposity. This is consistent with the known increased breast cancer risk associated with obesity. Excessive body adiposity may have provided a systemic and local environment that is conducive for BC initiation and progression. The opposite impacts of body adiposity on TN and TP BC in some age groups suggests that the development of BC in slim women needed to be boosted by the expression of all hormone and HER-2 receptors, while BC might prevail in obese women without the aid of any receptors. Our results also suggested that DCIS patients in the 30 – 49 age range had lower body adiposity with respect to those with invasive BC. This raised the possibility that low body adiposity may help to prevent the progression of BC from in-situ malignancy to invasive malignancy. Spearman’s rank analysis demonstrated that BMI is reasonably correlated with our surrogate body adiposity marker, the thickness of the UAAL. The small discrepancy between BMI and the thickness of the UAAL may be due to the inherent individual body fat distribution variation.Conclusion
Breast cancer is significant associated with age and body adiposity. Particularly, breast cancer patients in the 50 – 59 age group had significantly higher body adiposity. The highly aggressive triple negative breast cancer was also associated with increased body adiposity. Lower body adiposity may help to limit the spreading of DCIS to become invasive breast cancer in some patients. Proper control of obesity remains a viable breast cancer prevention measure.Acknowledgements
National Cancer Institutes CA154738References
1. Zhu W, Huang P, Macura KJ, Artemov D. Association between breast cancer, breast density, and body adiposity evaluated by MRI. Eur Radiol. 2016;26:2308-2316.
2. Zhu W, Harvey S, Macura KJ, Euhus DM, Artemov D. Invasive Breast Cancer Preferably and Predominantly Occurs at the Interface Between Fibroglandular and Adipose Tissue. Clin Breast Cancer. 2016.
Figures