4910
Detection of pulmonary perfusion deficits in patients with cystic fibrosis by means of Self-gated Non–Contrast-Enhanced Functional Lung (SENCEFUL) MRI1Institute for Diagnostic and Interventional Radiologiy, University Hospital Wuerzburg, Wuerzburg, Germany, 2Department of Pediatrics, University Hospital Wuerzburg, Wuerzburg, Germany
Synopsis
The study’s purpose was to assess the performance of Self-gated Non–Contrast-Enhanced Functional Lung (SENCEFUL)-MRI in detecting pulmonary perfusion deficits in patients with cystic fibrosis (CF). Nineteen patients with cystic fibrosis and 19 matched healthy controls underwent SENCEFUL-MRI at 1.5T. Four blinded readers rated perfusion and phase (i.e. temporal distribution of pulmonary blood flow) maps separately regarding local deficits followed by simultaneous assessment of both maps. Furthermore, phase data was plotted in histograms for objective comparison to the reader’s results. SENCEFUL-MRI revealed statistically significant differences between CF-patients and controls. Furthermore, it demonstrated its potential in detection of pulmonary perfusion deficits.
Introduction
SENCEFUL (SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging)-MRI generates ventilation and perfusion data without the need for breath-holds or administration of contrast media (1). It has been demonstrated to reliably assess pulmonary ventilation impairment in patients with cystic fibrosis (CF) with high spatial resolution (2). In particular, this study found CF-patients to show a specific distribution pattern of small ventilation defects predominantly affecting the upper lobes and in part without any ventilation impairments in single maps or quadrants, corresponding well with previous publications describing an inhomogeneous pulmonary affection most often involving the upper lobes more heavily (3). Moreover, impaired ventilation is known to lead to perfusion defects even in very early stages of CF in part before structural changes to the lung are visualized. Wielpütz et al. showed that perfusion alterations can be detected within the first year of life in many patients, albeit only with contrast-enhanced MRI (4). Study purpose was to assess performance of SENCEFUL-MRI in detecting deficits in pulmonary perfusion and pulmonary perfusion phase (i.e. data regarding the temporal distribution of pulmonary blood flow) by examining patients with proven CF.Methods
A total of 38 participants, 19 patients with established CF-diagnosis and 19 healthy controls underwent SENCEFUL-MRI on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) equipped with a 32-channel body coil. SENCEFUL is based on a 2D fast low-angle shot (FLASH)-sequence utilizing quasi-random sampling. Cardiac and respiratory self-navigation is established by additional acquisition of four data points in the k-space center (i.e. in absence of any encoding gradients). The resulting direct current signal (DC signal) allows for retrospective assortment of single phase-encoding steps to their respective position in respiratory and cardiac cycles. Technical details have been described in (1). Pulmonary signal alterations during cardiac and respiratory cycles are transferred to color-coded organ maps of the lung displaying either pulmonary perfusion or pulmonary perfusion phase data. Lungs were manually segmented and maps generated in coronary orientation with 10mm slice thickness, respectively. Four readers blinded to all clinical information rated a total of 1644 coronal lung maps. Lungs in each map were rated per quadrant using a 4-point Likert scale (1=healthy, 2=defect <25% quadrant area, 3=defect <50% quadrant area, 4=defect >50% quadrant area). Readers rated perfusion and phase maps separately followed by simultaneous assessment thereof. To assess heterogeneity of pulmonary blood flow, phase data was plotted in histograms and a subsequent Gaussian fit was performed. Based on the histograms, a peak-to-offset ratio was calculated as the maximum value of the fitted curve divided by the mean of the outer 10% values (5). T-testing was performed for statistical significance; interrater-reliability was determined by means of Intraclass-Correlation testing (ICC).Results
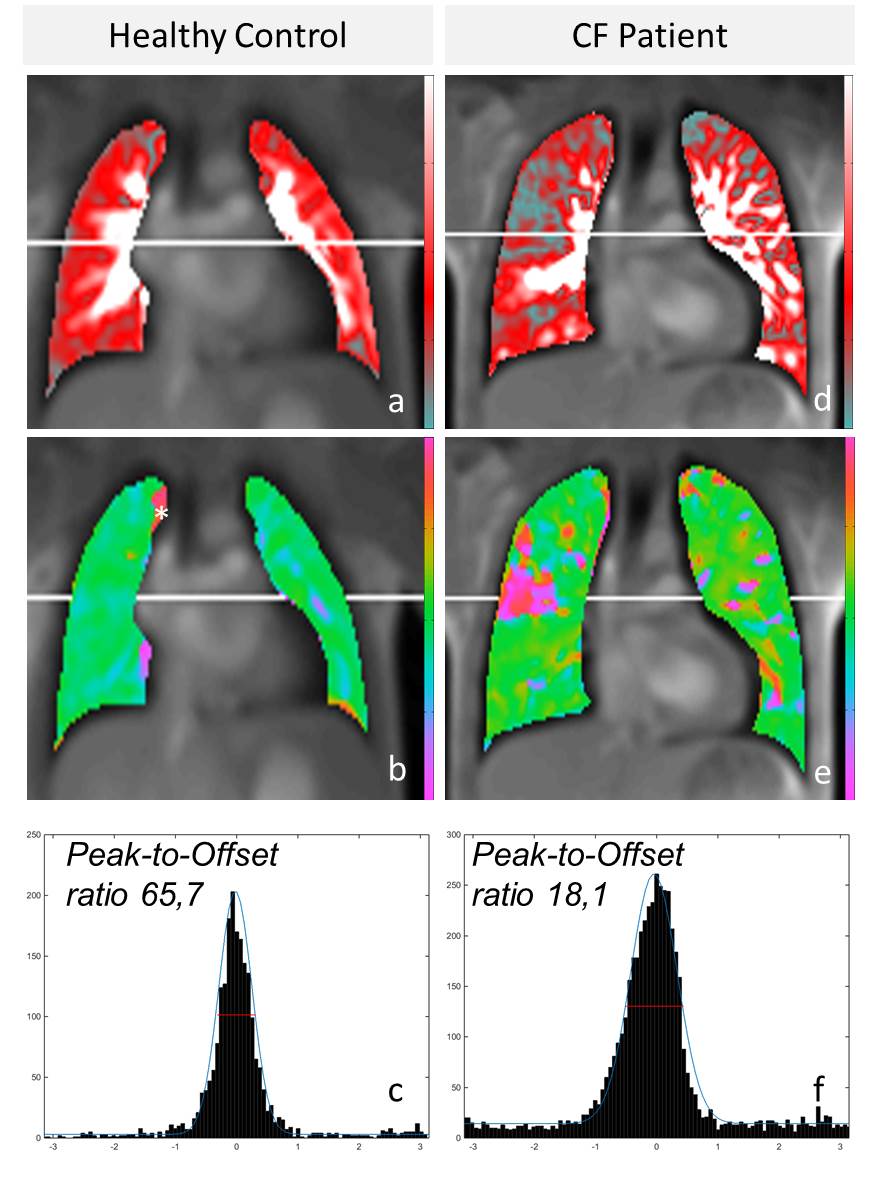
Figure 1 depicts exemplary maps of pulmonary perfusion, pulmonary perfusion phase and peak-to-offset histograms of a CF-patient and healthy control as utilized for analyses. Overall, in perfusion maps readers attributed pathological/conspicuous scores (i.e. scores of 2-4) to 25.3% of quadrants for the control-cohort vs. 56.5% for CF-patients (p<0.05). Phase maps were rated with pathological values in 20.9% for controls vs. 56.1% for CF-patients (p<0.05). Simultaneous assessment of perfusion and phase maps showed 15.1% pathological scores for controls vs. 53.6% for CF-patients (p<0.05). ICC-analysis for Inter-Reader-Agreement regarding the 4-point scale showed good agreement (perfusion: 0.85 phase: 0.81, combined: 0.82). Mean scores for perfusion maps were calculated at 1.35 (controls) vs. 1.98 (CF-group; p<0.05), for phase maps at 1.28 vs. 1.92 (p<0.05) and for simultaneous assessment at 1.21 vs. 1.90 (p<0.05). Histogram-based objective assessment of peak-to-offset ratios showed a median value of 63.8 in controls vs. 15.3 in CF-patients (p<0.05).Discussion
SENCEFUL MRI depicts lung perfusion and perfusion phase data without the need for breath-holds or contrast agents. Similar to afore published SENCEFUL-ventilation data for CF-patients (1), the perfusion-weighted data showed an inhomogeneous distribution of deficits throughout the lung. This constellation is well explainable by hypoxic vasoconstriction in areas of reduced ventilation, also known as the Euler-Liljestrand-Mechanism. Simultaneousl assessment of both perfusion and perfusion phase maps aided in discrimination of focal defects and objective evaluation by means of calculated peak-to-offset ratios of phase distribution data. A number of CF-patients showed single or multiple lung quadrants to be unimpaired suiting inhomogeneous disease distribution characteristics and/or mild courses of CF. Conversely, conspicuously rated quadrants of controls can be attributed to e.g. partial volume effects or through-plane motion.Conclusion
SENCEFUL MRI bears the potential for disease monitoring of CF. Its ability for high spatial resolution provides additional insight into focal distribution of defects or impaired areas of the lung and could conceivably aid in e.g. planning of bronchoscopic interventions.Acknowledgements
No acknowledgement found.References
(1) Fischer, et al. NMR Biomed. 27:907-917 (2014)
(2) Veldhoen, et al. Radiology 2016, Oct 6:160355, Epub ahead of print (2016)
(3) Brody, et al. J. Pediatric. 2004, Jul;145(1):32-8 (2004)
(4) Wielpütz, et al. Am J Respir Crit Care Med. 2014, Apr 15; 189(8):956-65 (2014)
(5) Veldhoen et al., Proc. Int. Soc. Mag. Reson. Med., 24:1144 (2016)
Figures