4860
Evaluation of unilateral obstructive uropathy using co-polarized 13C-pyruvate and 13C-urea1MR Research Centre, Skejby University hospital, Aarhus N, Denmark, 2Clinical institute, Skejby University hospital, Aarhus N, Denmark
Synopsis
Unilateral obstructive uropathy (UUO) is a cause of acute kidney injury and can also lead to chronic kidney diseases. A common cause for UUO is kidney stones and is also often the cause of end-stage renal diseases in children because of congenital development defects. Here we used a unilateral obstruction model with obstruction release after 5 days, and injection of co-polarized 13C-pyruvate and 13C-urea 2 days after release. We saw a marked elevation in lactate/pyruvate ration in the UUO kidney of the animals and also a reduction of approx. 50% in kidney blodflow measured by 13C-urea. The mechanisms involved must be investigated further. We believe that injection of co-polarized 13C-pyruvate and 13C-urea can be used as a clinical tool to follow kidney metabolic status and blodflow after surgical release of ureter obstruction.
Purpose
Unilateral obstructive uropathy (UUO) is a common cause of complex kidney disease, often caused by formation of kidney stones, which blocks the urine flow from the kidney. Ureteral obstruction is characterized by inflammatory cell infiltration, primarily by accumulation of macrophages in the obstructed kidney, accompanied with increased apoptosis and oxidative stress (1). Currently, there are few tools available to diagnose and monitor the progression of kidney injury after surgical release of UUO without causing further injury to the damaged kidney e.g. by ionizing radiation or contrast induced nephrotoxicity. By using co-polarized 13C-pyruvate and 13C-urea we are able to collected information about metabolic status and perfusion simultaneously with only one injectionMethods
One Wistar Rat (278 gram) was included in the pilot study. A midline incision in the abdomen was made and the left ureter was dissected carefully. A ligature was tied around the ureter with small plastic tubing along the ureter. The animal was sutured in the muscle and skin layer, 5 days after obstruction the ligature and plastic tubing was removed. Macroscopic observation revealed formation of much connective tissue and a full obstructive release was properly not formed. Temperature and respiration was monitored during the surgical procedure. 2 days after release surgery a tail vein catheter was inserted for injection of the co-polarised 13C-pyruvate and 13C-Urea. Temperature, arterial oxygen saturation and respiration rate were monitored throughout the experiment. The animal received one injection of 1.1 mL hyperpolarized solution over 10 s. The experiments were performed in a 3 T clinical MR system (GE Healthcare) equipped with a dual tuned 13C/1H volume rat coil. A slice-selective 13C IDEAL spiral sequence was used for hyperpolarized 13C-pyruvate and 13C-Urea imaging acquiring images every 5 s initiated 20 seconds after the start of injection. Flip angle=10º, 11 IDEAL echoes and one initial spectrum per IDEAL encoding, TR/TE/ΔTE=100 ms/0.9 ms/0.9 ms, FOV=80x80 mm2, 5 x 5 mm real resolution and an axial slice thickness of 15 mm covering both kidneys.Results and Discussion
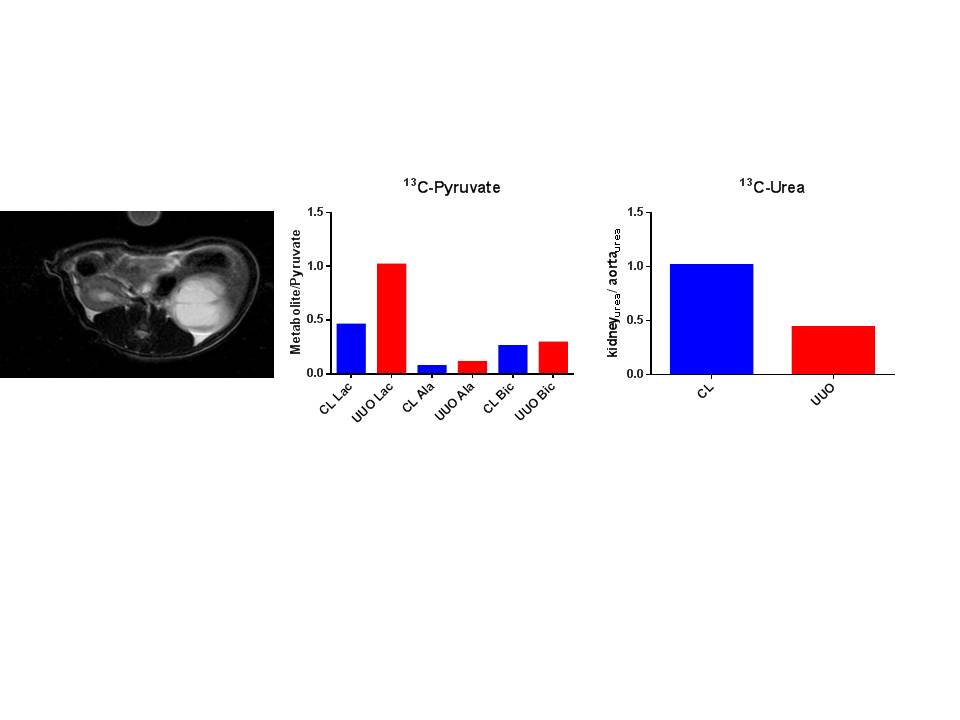
Interestingly, we found an elevated lactate/pyruvate ratio in the UUO kidney compared to the contralateral kidney indicating elevated anaerobic metabolism in the UUO kidney, as these measurements only have been performed in one animal, no direct conclusion can be drawn. A very small tendency for elevation is also seen in the alanine/pyruvate and bicarbonate/pyruvate ratio, albeit this is by no means conclusive. The 13C-urea data clearly indicate a reduction in blodflow to the UUO kidney, this is in agreement with a study performed by Niles et. al. (2). This might suggest that total ureter release was not yet formed or that the kidney needs more time to normalize. Also proton images revealed a still very edematous UUO kidney. We propose that the reduced blood flow to the UUO kidney is the cause for an upregulation of the anaerobic pathway, as a reduced blodflow is followed by a reduction in oxygen delivery.Conclusion:
In conclusion we were able to polarize two molecules in the same fluid path. This gave rise to information concerning both metabolism and perfusion in the same scan session. Interestingly there is an apparent increase in the lactate/pyruvate ratio in the UUO kidney compared to the contralateral kidney. Also perfusion is severely reduced in the UUO kidney which is seen from the 13C-urea data. Therefore we propose that reduced oxygen delivery to the UUO kidney is causing the elevation in anaerobic metabolism.Acknowledgements
Henrik Vestergaard is acknowledged for his laboratory assistance.References
1. Dendooven A, Ishola DA,Jr, Nguyen TQ, Van der Giezen DM, Kok RJ, Goldschmeding R and Joles JA. Oxidative stress in obstructive nephropathy. Int J Exp Pathol 92: 202-210, 2011
2. Niles DJ , Jeremy GW , Smith MR , Reese S , Djamali A , Sadowski EA , Fain SB. Evaluation of the progression of obstructive nephropathy in a UUO mouse model using BOLD, hyperpolarized 13C, and DCE MRI. Proc. Intl. Soc. Mag. Reson. Med. 20, 2012
Figures