4840
Can Thoracic MRI Add Value to Your Practice?1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
After reviewing state-of-the art clinical applications of thoracic MRI, reader will become cognizant of potentials and limitations of thoracic MRI and be the judge of whether thoracic MRI can add value to clinical practice.
Can Thoracic MRI Add Value to Your Practice?
Learning Objectives:
1. Identify recent advancements of thoracic MRI including PET/MRI.
2. Describe nonvascular clinical applications of MRI in the thorax.
3. Discuss advantages and limitations of MRI compared to commonly used modalities.
Since the clinical introduction of magnetic resonance imaging (MRI), thoracic application has been technically challenging due to inherent properties of the lung parenchyma and motion artifacts from physiologic excursion of the heart and lungs. However, proton MRI has experienced tremendous growth within the past decade due to improved scanners and coils, technical advances in sequencing and post-processing, and utilization of contrast media. State-of-the art thoracic MRI now has the potential to supplement traditional imaging techniques in patient management.
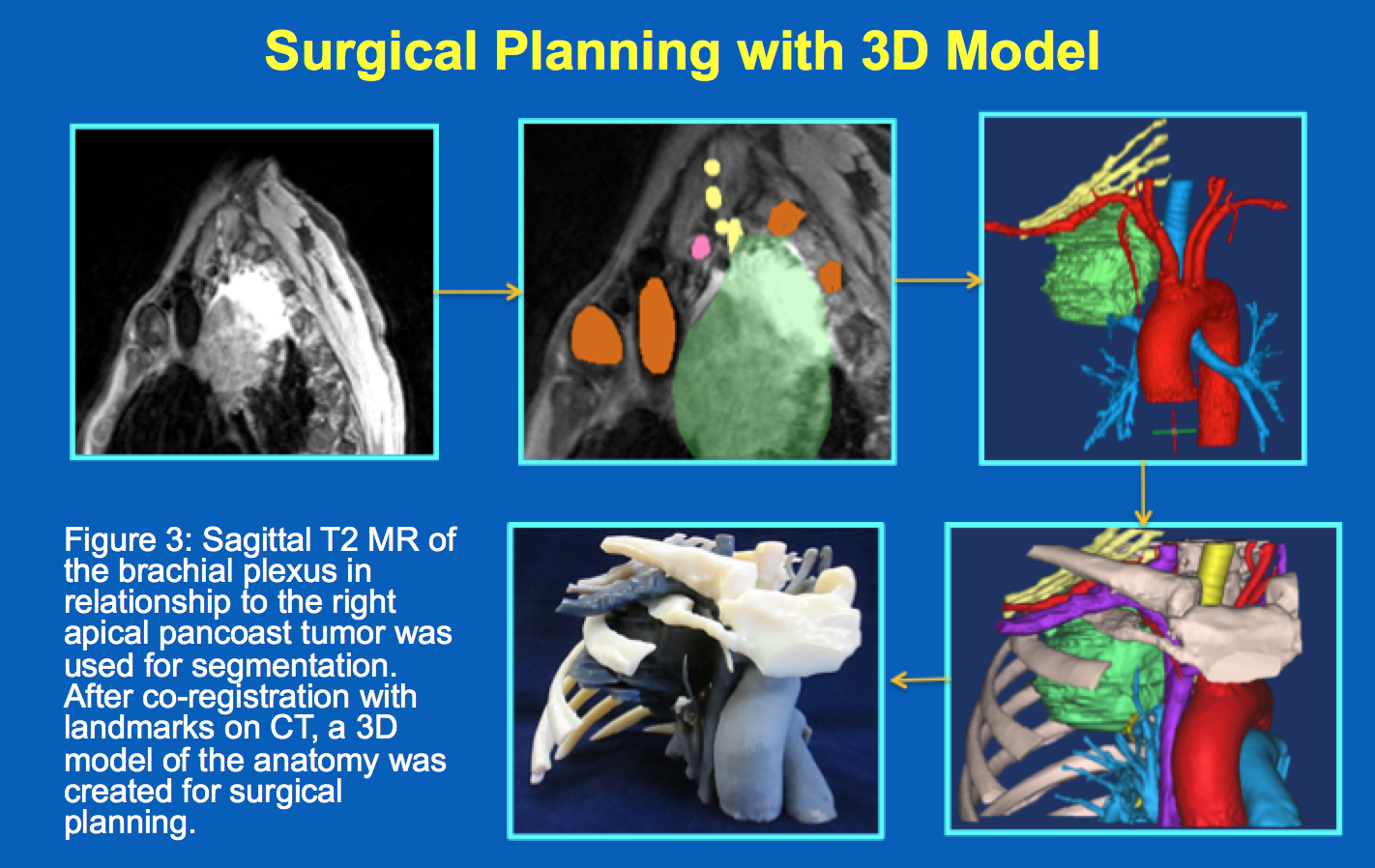
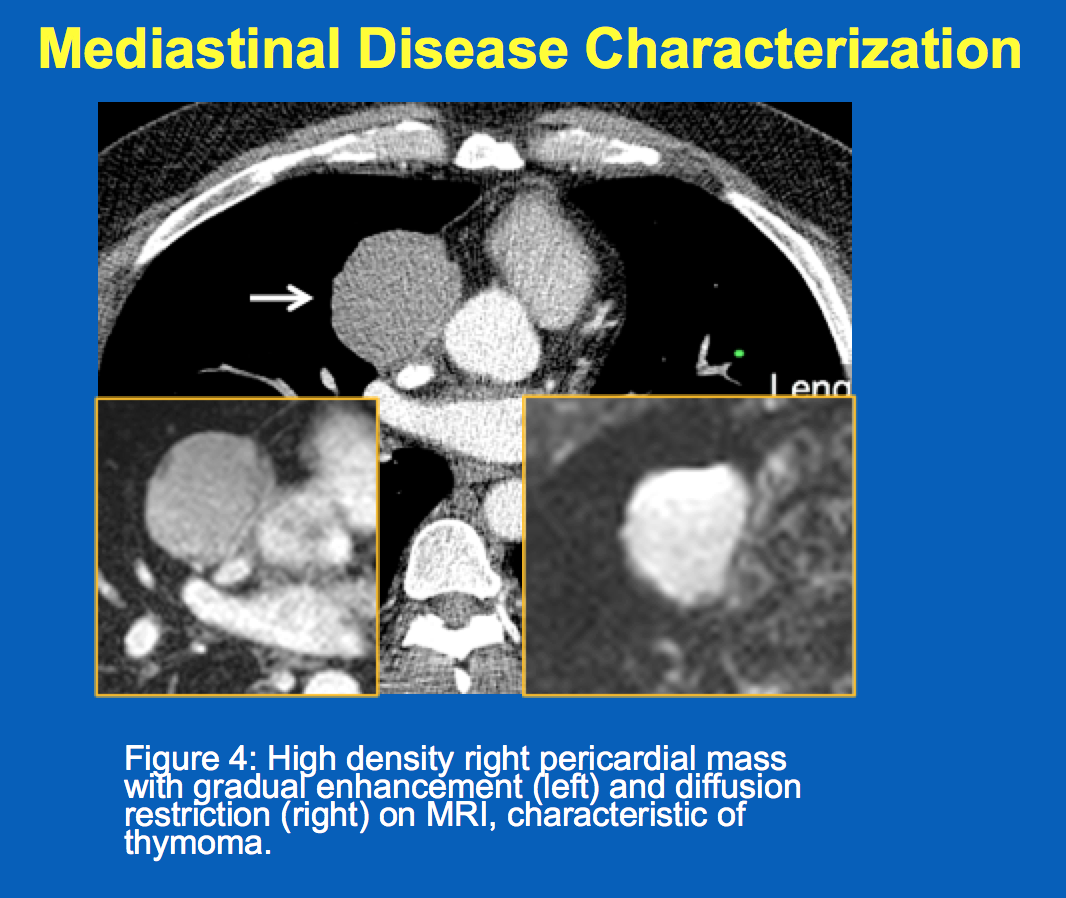
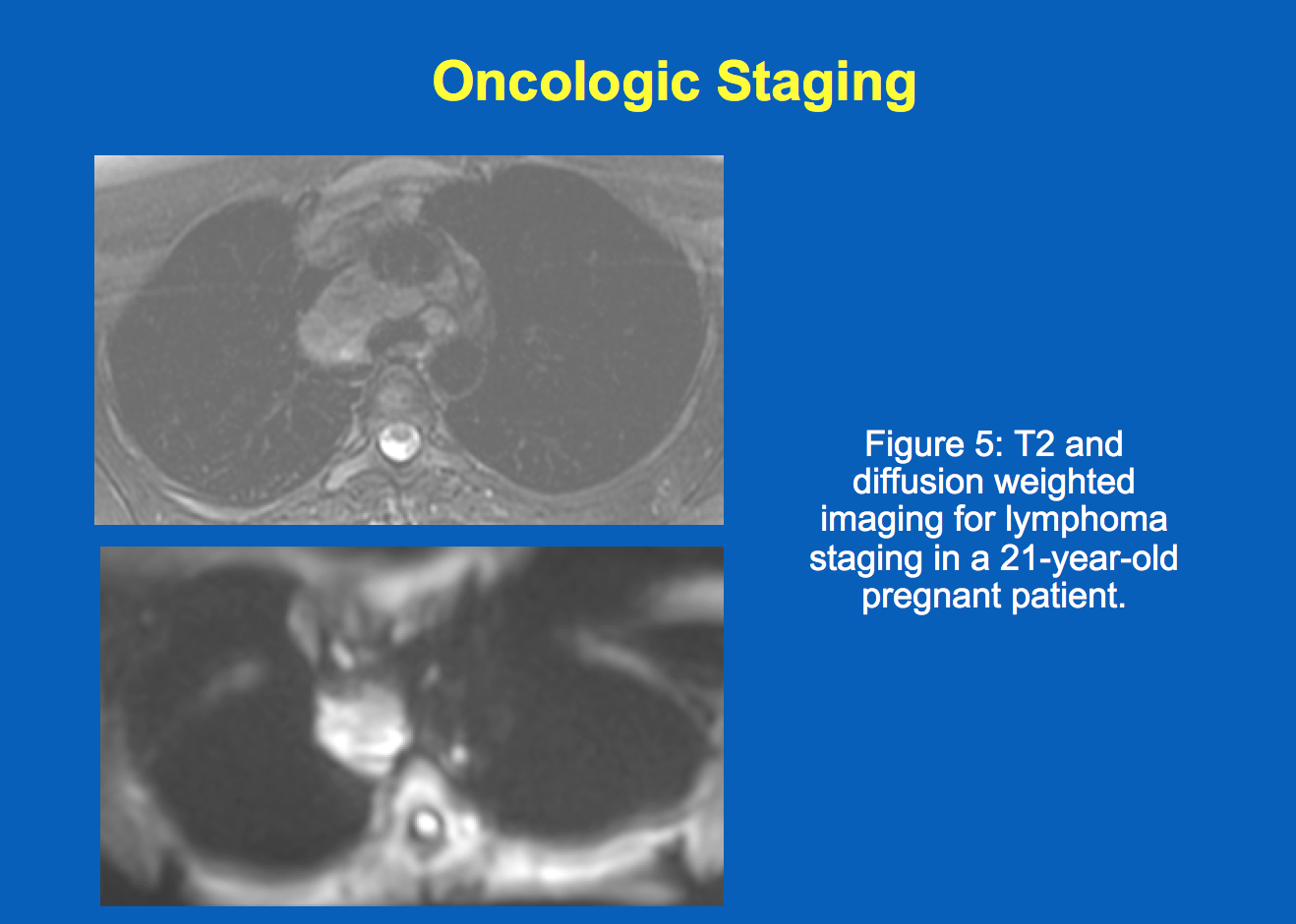
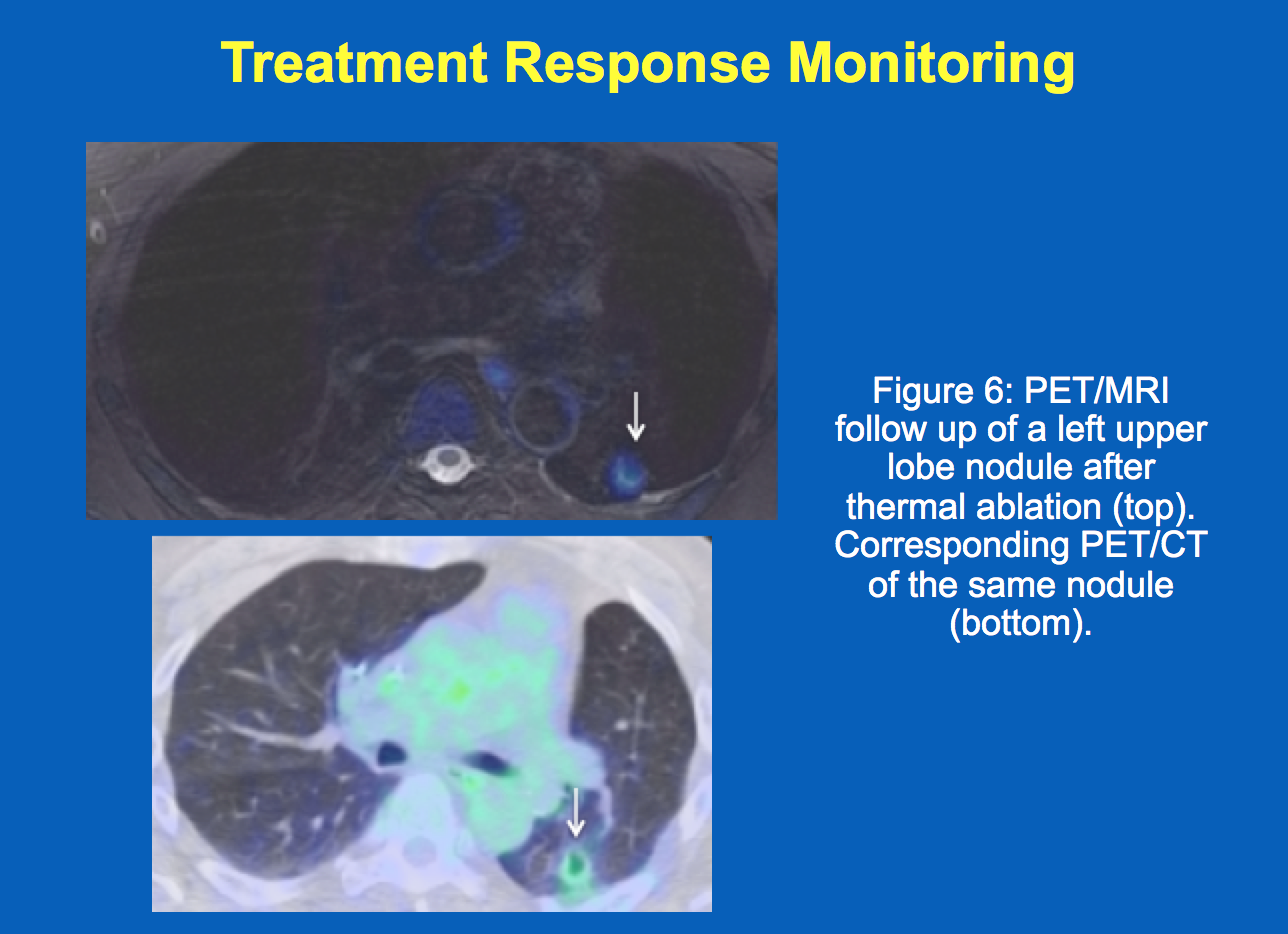
In this review, we focus on several advances in thoracic MR imaging and highlight novel applications in pulmonary nodule assessment, cancer staging, mediastinal and pleural disease evaluation, radiation planning and surgical planning utilizing 3D modeling. We will also discuss strengths and weaknesses of MR thoracic imaging compared to conventional modalities. Familiarity with the potentials and limitations of clinical application of thoracic MRI can set forth goals for MR developers to generate more robust techniques for imaging the thorax. The potential paradigm shift towards thoracic MRI renders for an exciting time for all in thoracic imaging.
Acknowledgements
No acknowledgement found.References
No reference found.Figures
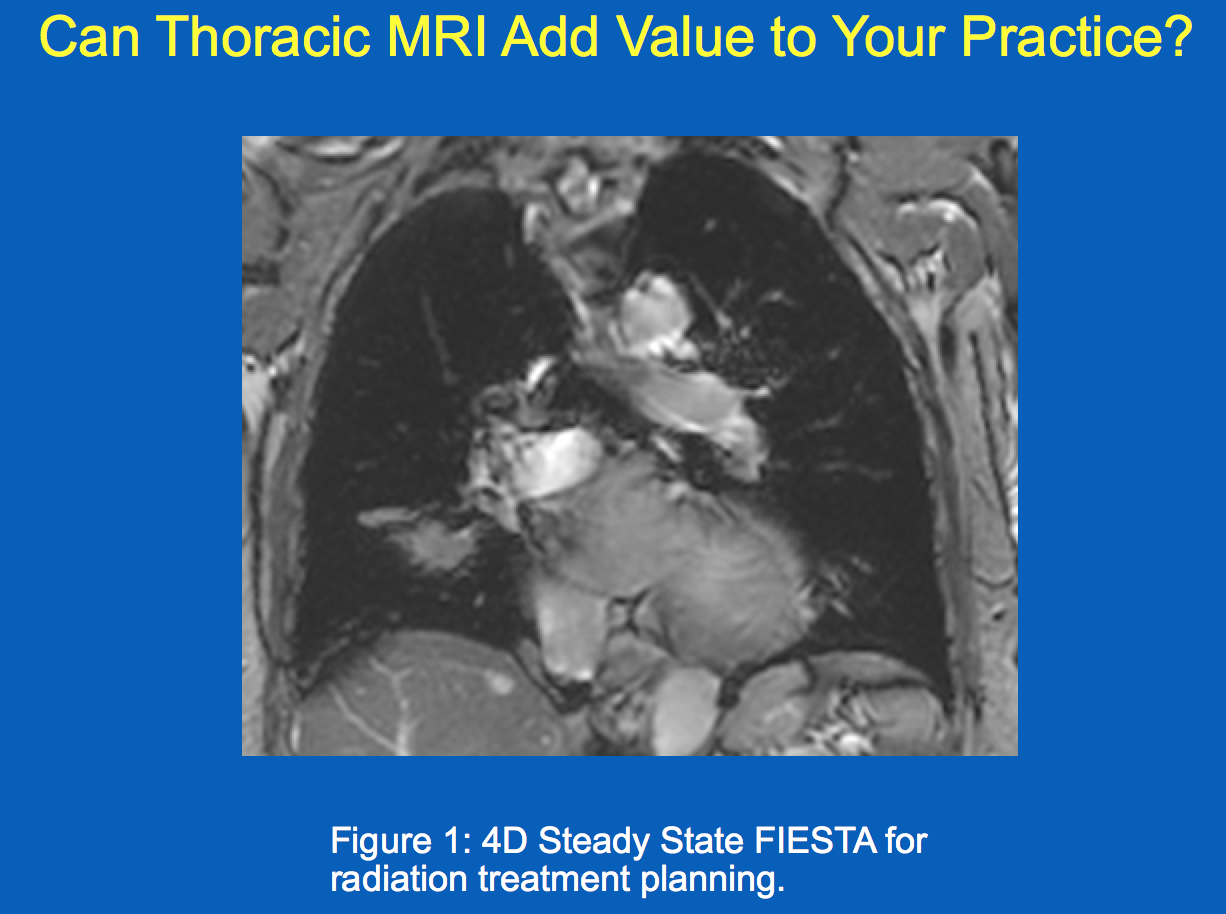
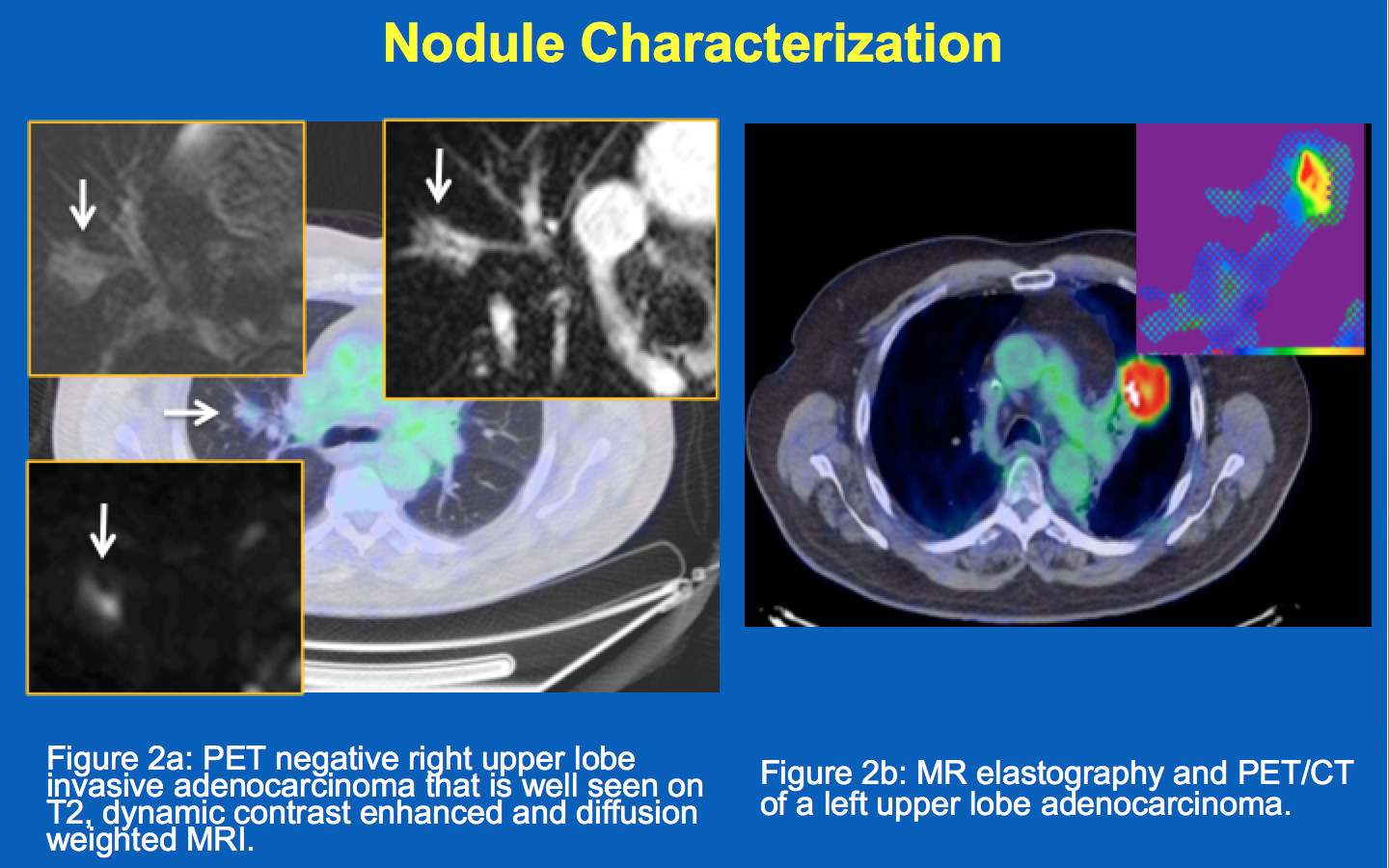
Figure 2a: PET negative right upper lobe invasive adenocarcinoma that is well seen on T2, dynamic contrast enhanced and diffusion weighted MRI.
Figure 2b: MR elastography and PET/CT of a left upper lobe adenocarcinoma.