4825
Whole body functional and anatomical MRI: Accuracy in staging of Childhood and Adolescent Hodgkin’s Lymphoma compared to conventional multimodality imaging1University College London, London, United Kingdom, 2University College London Hospital, London, United Kingdom
Synopsis
Current gold standard imaging for assessment of paediatric Hodgkin's lymphoma is PET-CT. Anatomical and functional whole-body MRI (WB-MRI) provides an alternative/adjunct radiation free imaging technique.
The aim of this prospective single centre study is to investigate the diagnostic accuracy of WB-MRI against reference standard imaging for staging of paediatric Hodgkin's lymphoma.
Purpose
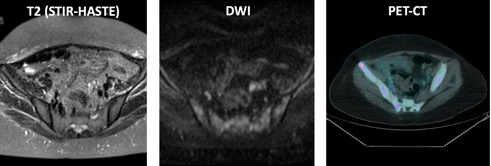
Positron emission tomography fused with computed tomography (PET-CT) +/- CT scan remains the gold standard imaging modality for staging of pediatric lymphoma despite the associated radiation risk [1]. Morphological whole-body MRI (WB-MRI) offers an alternative non-ionizing technique [2] that can be supplemented by functional imaging, notably diffusion-weighted imaging (DWI) for staging and assessment of extent of the disease [3]. The aim of this study was to prospectively assess the agreement between multi-parametric whole-body MRI (WB-MRI) and conventional investigations for staging of childhood Hodgkin’s lymphoma (HL).Materials and methods
Fifty-eight patients with a confirmed new diagnosis of HL underwent WB-MRI in addition to conventional CT and PET-CT at initial staging. The combined reference standard (CRS) assessment for disease stage was undertaken by a multidisciplinary team (MDT) committee based on all clinical and imaging data including PET CT and CT, using the EURONET trial criteria (nodal positivity >2cm and/or focal 18-FDG uptake above background). Twenty-two disease sites (11 nodal, 11 extra nodal) were assessed for the presence of disease and patients were staged according to Ann Arbor system The WB-MRI (1.5 T, Avanto, Siemens healthcare) assessment included axial/coronal FS T2/T1 TSE, axial FS DWI (5 b values 0 to 800), and dynamic contrast enhanced T1 FLASH through the liver/spleen. Based on pilot data, nodal positivity was defined as long axis diameter >2cm and/or mean ADC < 1.2 x10-3mm2 s-1. Nodes 1 to 2cm with ADC 1.2-1.8 were equivocal. WB-MRI imaging was assessed for the same 22 disease sites in consensus by 2 radiologists blinded to all conventional imaging and clinical data. To improve the robustness of the CRS, an unblinded consensus committee (radiologist, nuclear medicine physician and oncologist) re-reviewed all baseline, follow-up imaging and clinical data and corrected the CRS for perceptual errors by original reporting doctors (eg during PET-CT reporting) and technical imaging errors (eg proven chest wall invasion not visible on CT) to derive an “enhanced CRS” (figure 1,2). Thereafter, WB-MRI data was retrospectively corrected for reader perceptual errors to define the theoretical best performance of the technique. Absolute agreement rate, true positive rate (TPR) (sensitivity), false positive rate (FPR) (1-specificity) and kappa statistic for both nodal and extra-nodal disease sites were derived for WB-MRI against CRS and enhanced-CRS. Equivocal sites were treated as disease positive. Also, the percentage of nodal and extra-nodal site concordance was calculated per patient where 100% concordance represents correct disease classification of all 11 disease sites respectively, 91% concordance represents correct classification of 10/11 disease sites and so on. The final Ann-Arbor staging agreement between CRS and WB-MRI was assessed using Kappa statistic.Results
Of 58 patients, 50 patients were evaluable. Amongst the evaluable patients, the median age was 16 years (range: 6 to 19) with 32 (64%) male. Figure 1 presents the agreement parameters for all reported nodal and extra-nodal disease sites between WB-MRI against the CRS, and enhanced CRS before and after removal of MRI perceptual errors. The median per patient concordance for WB-MRI against the enhanced CRS was 100% (IQR 94 to 100%) and 100% (IQR 97 to 100%) for nodal and extra nodal disease sites respectively. When WB-MRI was corrected for perceptual errors and compared with enhanced CRS, a total of 42/50 (84%) and 46/50 (92%) of patients were fully concordant for each of the 11 nodal and extra nodal site respectively There was 68% (34/50) agreement for Ann-Arbor staging, (kappa 0.52 95%CI 0.35-0.69-moderate), with 10 (20%) patients under staged by WB-MRI and 6 (12%) over staged. However, against the enhanced reference standard and following the removal of WB-MRI perceptual errors, the agreement increased to 92% for staging (kappa, 0.93 95%CI:0.76-0.99- almost perfect). Figure 2 and 3 demonstrate two cases with discrepant staging. After correcting for perceptual errors and compared to enhanced reference standard, 2 (4%) patients were down-staged and 1 (2%) patient up-staged by WB-MRI.Discussion and Conclusion
This prospective study suggests WB-MRI has considerable promise as an alternative radiation-free technique to conventional staging modalities such as PET CT, with reasonable agreement between staging modalities. However absolute concordance varies between 84 and 92% for nodal and extranodal disease respectively even after correcting for WM-MRI perceptual errors suggesting caution must be taken before introducing into staging algorithms as a replacement test.Acknowledgements
No acknowledgement found.References
[1] Chawla SC, Federman N, Zhang D, et al, Estimated cumulative radiation dose from PET/CT in children with malignancies: a 5-year retrospective review. Pediatr Radiol 2010;40: 681-686.
[2] Punwani S, Taylor SA, Bainbridge A, et al. Pediatric and adolescent lymphoma: comparison of whole-body STIR half-Fourier RARE MR imaging with an enhanced PET/CT reference for initial staging. Radiology 2010; 255:182-190.
[3] Kwee TC, Takahara T, Vermoolen MA, et al. Whole-body diffusion-weighted imaging for staging malignant lymphoma in children. Pediatr Radiol 2010 40:1592-1602.
Figures
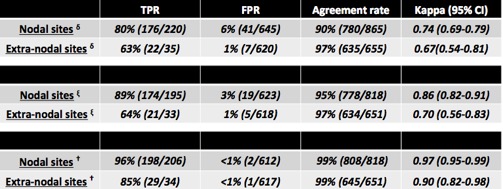
Figure 1: Agreement between whole-body MRI and combined reference standard
TPR: true positive rate, FPR: false positive rate, 95%CI: 95% confidence interval
δ Agreement between WB-MRI and uncorrected combined reference standard
ξ Agreement between WB-MRI and enhanced combined reference standard prior to removing WB-MRI perceptual errors
† Results comparing WB-MRI with enhanced combined reference standard after removing WB-MRI perceptual errors