4823
Potential of parallel transmission for fetal imaging in reducing SAR and mitigating flip angle inhomogeneities: a simulation study at 3T1Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, MA, United States, 2Fetal-Neonatal Neuroimaging & Developmental Science Center, Boston Children's Hospital, Harvard Medical School, Boston, MA, United States, 3Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 4Department of Radiology, Harvard Medical School, Boston, MA, United States, 5Harvard-MIT Division of Health Sciences and Technology, Massachusetts Institute of Technology, Cambridge, MA, United States, 6Institute for Medical Engineering and Science, Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
In this work we evaluate the potential benefits of parallel transmission for fetal imaging in reducing local SAR and mitigating flip angle inhomogeneities. Our results show that compared to single channel transmission, using 2 channel parallel transmission with a 2 port birdcage coil, local SAR can be reduced by a factor of up to 5 and flip angle inhomogeneity can be mitigated by up to 66% for realistically long RF pulses.
PURPOSE
This work is a preliminary study on evaluating the potential of parallel transmission (pTx) technology in addressing the RF safety/limitation as well as flip angle inhomogeneity concerns associated with fetal imaging at 3T. Standard fetal protocols include several HASTE scans that are specific absorption rate (SAR) intensive which results in limitations in imaging time. Moreover, even when operating under the safety limits suggested for adults, several studies so far expressed their concern on the safety of the fetus (1-4). Furthermore, fetal imaging also suffers from flip angle inhomogeneities across the large pregnant torso at 3T. One study by Filippi et. al. experimentally showed image uniformity improvement and global SAR reduction in fetal imaging using 2 channel RF transmission (5). However, only global SAR was considered in that study for ensuring safety. Another study by Murbach et. al. explores RF shimming to improve field inhomogeneity (6). The non-uniformity is improved by 12% with reduced SAR in the mother however increased SAR is observed for the fetus. In that study, a greedy search algorithm is applied to cover all phase and magnitude combinations without any constraints on local SAR. In this study we implement an explicitly local SAR constrained pTx pulse design algorithm for fetal imaging at 3T using 2 channel RF transmission. Our findings show significant reduction in local SAR, and the flip angle uniformity compared to the standard birdcage mode of operation.METHODS
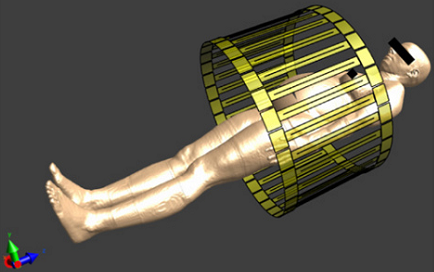
EM Simulations: A pregnant body model with 7 month gestational age (7) is simulated inside the 2-port, 32-rung birdcage Skyra coil model (Siemens Healthcare, Erlangen, Germany) using Sim4Life (ZMT, Zurich, Switzerland) to obtain the electromagnetic fields (Figure.1). The body model is positioned to center the fetus brain at the isocenter of the coil. The matchings of the ports are less than -14 dB when loaded with the pregnant body model. The resulting B1+ field has a max/min ratio of 2.9 in the isocenter slice inside the body model.
Pulse Design: The electric fields are extracted and the computed SAR matrices in the body are compressed into virtual observation points (VOPs) (8). The VOPs and the B1+ fields are fed into a slice selective high flip angle local and global SAR constrained RF pulse design algorithm using magnitude least squares (MLS) optimization (9) to design 90° excitation as well as 180° refocusing pulses. A Hanning windowed sinc subpulse with a time bandwidth product of 2 and a duration of 4.1 ms (2.1 ms) is chosen for the refocusing (excitation) pulses. A duty cycle of 10% was assumed in calculating the SAR values. The standard circularly polarized birdcage mode pulse is scaled to give an average flip angle of 90° and 180° for a more fair comparison of the pulse performances. For the same purpose, a second CP BC mode pulse whose pulse length is matched to the 2 spoke pTx pulse is evaluated. Off resonance is assumed to be zero, which is an assumption that gets worse as the pulse duration becomes longer (2 spoke pulses).
RESULTS
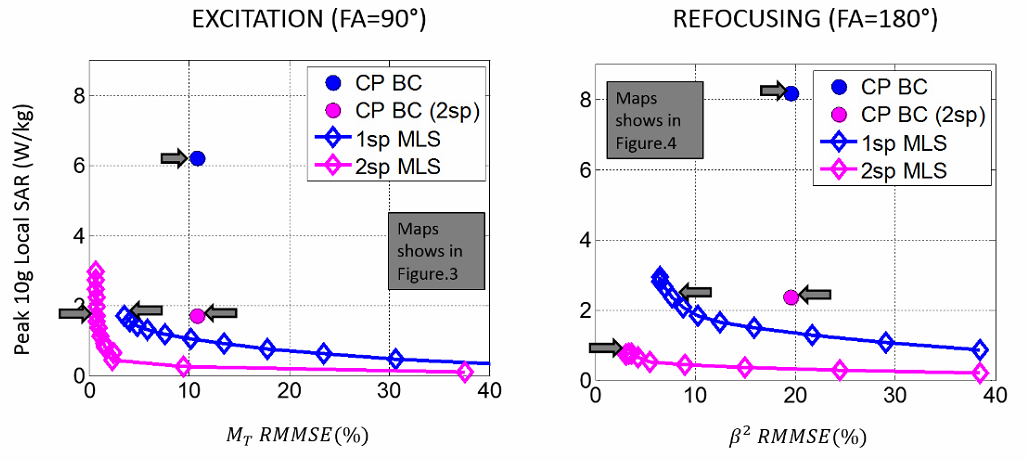
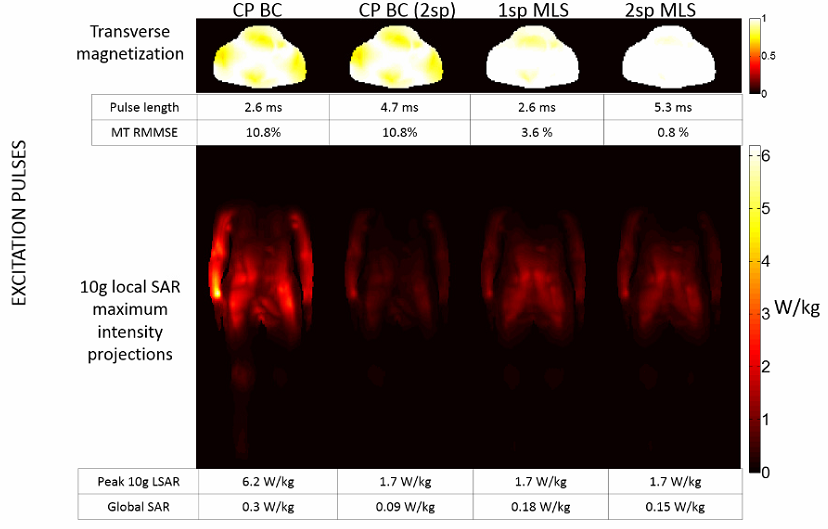
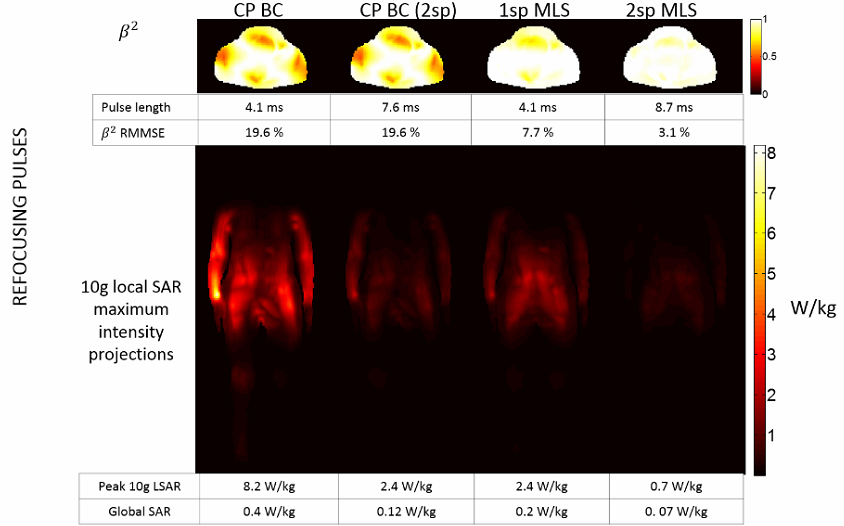
Figure.2 shows the excitation/refocusing uniformity vs local SAR tradeoffs for various pulse designs as well as the standard BC pulses. Peak 10g averaged local SAR can be reduced by a factor of up to 5 and 6.5 for excitation and 5.3 and 7.5 for refocusing pulses using 1 and 2 spoke pulses. Furthermore, the excitation (refocusing) fidelity can be improved by up to 66% and 94% (66% and 85%) using 1 spoke and 2 spoke MLS pulses compared to the standard mode of operation. (Fig.3, Fig.4 first rows). However, note that off resonance is assumed to be zero and hence the 2 spoke pulse performances will degrade significantly in the presence of B0off due to their long duration especially for refocusing pulses. The maximum intensity projections for local SAR show that local SAR hot spots are usually located around the arms for CP BC and torso for spokes pulses, which is consistent with (6, 10). The global SAR is lower than 2W/kg for all cases.DISCUSSION
This study suggests parallel transmission, as in non-pregnant imaging, is a powerful tool to improve fetal imaging at 3T. For the 2 port Skyra coil, both the local SAR and the flip angle non-uniformity can be significantly and simultaneously reduced. The reduced local SAR implies a reduced temperature increase. However, local SAR and temperature are not linearly related. Therefore, future work will focus on temperature simulations. Moreover, the effect of choosing an ROI around the fetus head as well as fetus friendly excitation modes will be explored.Acknowledgements
This work was supported by R01 EB017337, R01 EB006847, P41EB015896, U01 HD087211, Siemens MR, and the Sim4Life support group.References
1. Kikuchi S, Saito K, Takahashi M, Ito K. Temperature elevation in the fetus from electromagnetic exposure during magnetic resonance imaging. Phys Med Biol 2010;55(8):2411-2426.
2. Hand JW, Li Y, Hajnal JV. Numerical study of RF exposure and the resulting temperature rise in the foetus during a magnetic resonance procedure. Phys Med Biol 2010;55(4):913-930.
3. Pediaditis M, Leitgeb N, Cech R. RF-EMF exposure of fetus and mother during magnetic resonance imaging. Phys Med Biol 2008;53(24):7187-7195.
4. Cannie M. Potential Heating Effect in the Gravid Uterus by Using 3-T MR Imaging Protocols: Experimental Study in Miniature Pigs. Radiology 2016;000(0).
5. Filippi CG, johnson A, Nickerson JP, Sussman B, Gonyea J, Andrews T. Fetal Imaging with Multitransmit MR at 3.0T Preliminary Findings. 2010. p 2023.
6. Murbach M, Neufeld E, Samaras T, Córcoles J, Robb FJ, Kainz W, Kuster N. Pregnant women models analyzed for RF exposure and temperature increase in 3T RF shimmed birdcages. Magnetic resonance in medicine 2016.
7. Marie-Christine Gosselin, Esra Neufeld, Heidi Moser, Eveline Huber, Silvia Farcito, Livia Gerber, Maria Jedensjo, Isabel Hilber, Fabienne Di Gennaro, Bryn Lloyd, Emilio Cherubini, Dominik Szczerba, Kainz; W, Kuster N. Development of a New Generation of High-Resolution Anatomical Models for Medical Device Evaluation: The Virtual Population 3.0 Physics in Medicine and Biology 2014;59(18):5287-5303.
8. Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med 2011;66(5):1468-1476.
9. Setsompop K, Wald LL, Alagappan V, Gagoski BA, Adalsteinsson E. Magnitude least squares optimization for parallel radio frequency excitation design demonstrated at 7 Tesla with eight channels. Magn Reson Med 2008;59(4):908-915.
10. Guerin B, Gebhardt M, Serano P, Adalsteinsson E, Hamm M, Pfeuffer J, Nistler J, Wald LL. Comparison of simulated parallel transmit body arrays at 3 T using excitation uniformity, global SAR, local SAR, and power efficiency metrics. Magn Reson Med 2015;73(3):1137-1150.
Figures