4818
Radial segmented echo-planar readout for fast fetal angiography – feasibility test1Department of Biomedical Engineering, Wayne State University, Detroit, MI, United States, 2Department of Radiology, Wayne State University, Detroit, MI, United States, 3Department of Obstetrics and Gynecology, Wayne State University, Detroit, MI, United States, 4Perinatology Research Branch, NICHD/NIH/DHHS, Bethesda, MD, United States
Synopsis
A simulation study showing the potential benefit of a radial-trajectory based data acquisition technique named as "radial segmented echo-planar readout (radialSEPI)" for faster fetal angiography is presented. The results indicate that at echo train length of 2 and echo-spacing of 6.1 ms can provide good quality fetal/adult MRA reconstructions providing a potential factor 2 improvement in time.
Background
Non-contrast magnetic resonance angiography (MRA) of fetal and placental vasculature has been reported recently using an optimized 2D time-of-flight sequence with Cartesian sampling of k-space1. Cartesian sampling trajectories, in general, are more susceptible to motion, compared to non-Cartesian trajectories, like radial, which densely sample the centre of k-space. However, it takes 1.5 times more read-out lines in radial trajectory, compared to Cartesian trajectory, for satisfying Nyquist sampling condition for a given voxel size and field-of-view2. Hence, strategies for speeding up radial trajectory data acquisition are of interest, especially in the context of fetal imaging where fast imaging is highly desired. For high contrast applications like contrast-enhanced MRA, previous works have shown that even with sub-Nyquist sampling at 128 or 200 spokes provide high quality data3. Further reduction in the data acquisition time is possible with multi-spoke readouts within one TR4. This approach is often dubbed as radial segmented echo-planar readout (radialSEPI). Through simulation studies using a double-echo flow-compensated radial MRA data from the adult and fetus, in this work we evaluate the image quality achievable using such a radialSEPI scheme.Material and Methods
After obtaining the informed consent in accordance with the local institutional review board guidelines, data was also acquired from one healthy adult volunteer and one adult pregnant subject in third trimester with normal, singleton pregnancy. All the scans were performed at 3.0T MRI (Siemens, Verio, Erlangen, Germany). The following MRI scan parameters were used in adult volunteer: readout points (Np) = 360, number of projections (Nr) = 720, TEs = 5.7 and 11.6 ms, TR = 22 ms, flip angle (FA) = 50°, resolution = 0.48×0.48×2 mm3, bandwidth(BW) = 241Hz/pixel, number of slices = 24 and in the fetus: Nr = 702, Np = 361, slices = 48, TR = 22 ms, FA = 500, TE = 5.7 and 11.6 ms, BW = 245Hz/px, resolution = 0.52x0.52x2 mm3. Both the first (TE1 (100%)) and the second echoes (TE2(100%)) were flow-compensated and 360 projections were acquired with golden angle (GA) increment. RadialSEPI data with a total of 360 (or 361) spokes was generated by taking the first 180 spokes from the first echo (TE1(50%)) and the subsequent 180 spokes from the second echo (TE2(50%)). Since the data was acquired with GA increment, irrespective of the TE, spokes from both echoes spanned all 4 quadrants of k-space. Magnitude data was then reconstructed according to the procedure outlined by4 (see Figure-1). Maximum intensity projections (MIPs) were generated from these simulated radialSEPI images and were visually compared with the full radial data from the first echo at 361 (or 360) spokes (TE1(100%)).Results
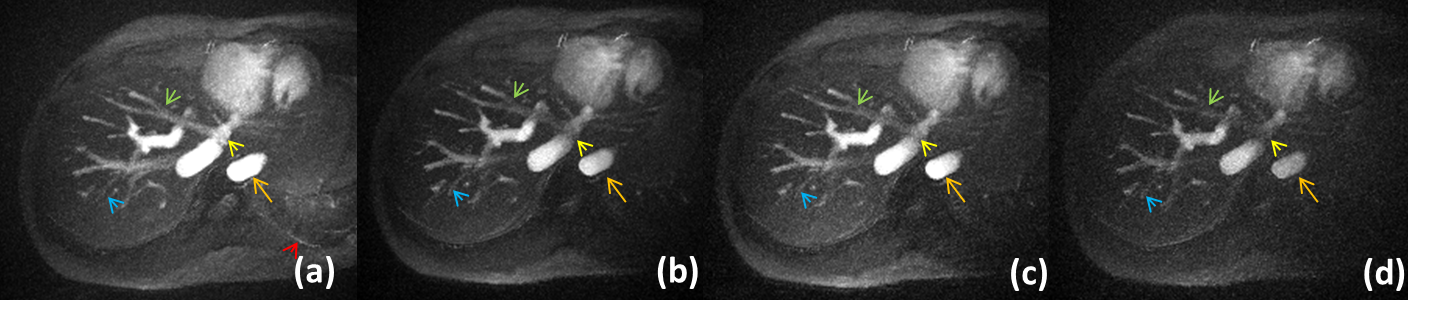
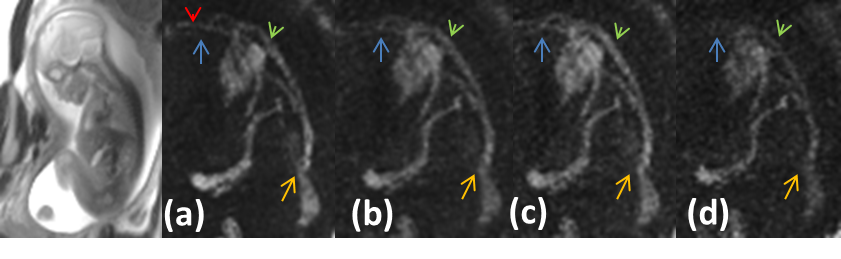
Figure-1 compares radialSEPI reconstruction with the TE1 reconstruction from full k-space (TE1(100%)). MIPs over 40 mm showing the portal vessels in an adult subject was taken for comparison. While the major vessels like the aorta and the inferior vena cava show higher amplitude signal from TE1(100%) data, compared to the radialSEPI image, overall vessel definition and visibility for both big and small vessels remain intact in radialSEPI reconstruction. Vessels on the order of a 1 to 2 pixels are however, not clearly visible in radialSEPI compared to TE1(100%) data. Figure-2 shows a similar comparison for major thoracic and abdominal vessels in a third trimester fetus (gestational age: 27 5/7 weeks). The TE1(100%) data represents fetal heart, the aortic arch, inferior vena cava as well as the umbilical vein. With radialSEPI reconstruction from TE1(50%) and TE2(50%) datasets, these large vessels remain clearly visible. However, the first branches of the aortic arch, which are on the order of a two voxels in diameter, are not clearly visible in radialSEPI as compared to TE1(100%).Discussion and Conclusion
This is a simulation study evaluating potential benefits of flow-compensated dual radial spoke readout within a given TR, for MR angiography application. The results indicate that at echo train length of 2 and echo-spacing as long as 6.1 ms can still provide good quality MRA reconstructions affording a potential factor 2 improvement in time. Exploring shorter echo-spacing and longer echo train lengths will be the focus of our future work. The actual sequence implementation itself will involve addressing the issue of eddy current and relative echo-shift (between different readouts) due to rapid gradient changes. Nevertheless, the results show that potential gain in the acquisition time without loss of image quality is possible and further decrease in echo-spacing should further improve the image quality. In conclusion, radialSEPI approach holds great potential for fast non-contrast angiography, in adults and especially in fetal imaging application.Acknowledgements
No acknowledgement found.References
1. Neelavalli, Jaladhar, et al. Magnetic resonance angiography of fetal vasculature at 3.0 T. European radiology (2016): 1-7.
2. Haacke, E. Mark, et al. Magnetic resonance imaging: physical principles and sequence design. Vol. 82. New York:: Wiley-Liss, 1999.
3. Peters, Dana C., et al. Undersampled projection reconstruction applied to MR angiography. Magnetic Resonance in Medicine 43.1 (2000): 91-101.
4. Winkelmann, Stefanie, et al. Simultaneous imaging and R2* mapping using a radial multi-gradient-echo (rMGE) sequence. Journal of Magnetic Resonance Imaging 24.4 (2006): 939-944.
Figures