4774
Free-Breathing cardiovascular imaging: comparing central k-space amplitude vs. phase based self-gating approaches1Department of Radiology, Wayne State University, Detroit, MI, United States, 2Department of Biomedical Engineering, Wayne State University, Detroit, MI, United States
Synopsis
Two self-gating approaches to reconstruct free-breathing cardiovascular image generated by Golden Angle radial trajectory MRI were compared. The results show that both central k-space magnitude and phase self-gated image have comparable quality with breathhold Cartesian CINE image, and the phase self-gating signal is less sensitive to the coil sensitivity compared to the magnitude based self-gating signal.
Introduction
When acquiring multiple slices through the heart in cardiovascular MRI (CMRI), successive breath-holds are typically needed which becomes (progressively) difficult as the number of slices increase. Free-breathing approaches with self-gating (SG) were developed to address this issue. Due to the time-of-flight effect from the blood motion, and/or changes in the structure of the heart during the cardiac cycle, the central k-space signal changes and thus can serve as the self-gating signal. Non-Cartesian trajectories, like radial trajectory, are widely used in self-gated 2D and 3D CMRI techniques.1, 2 While previous literature points out that both amplitude and the phase of the k-space center can be used for SG, results from amplitude-only based SG were reported.3, 4 In this work, we compare SG reconstructions based on amplitude versus phase of the k-space center in a gradient echo sequence with a radial sampling scheme. The motivation for exploring phase-only based SG is the difficulty introduced by phased array coil sensitivities. While amplitude signal is significantly modulated by spatially varying coil-sensitivities, phase on the other hand is less affected. We further evaluate whether a phase-only based SG (PSG) approach can resolve breathing versus heart motion which has been shown to be possible previously with amplitude based SG (ASG).2-4 Reconstruction efficacy between different approaches was evaluated by visual comparison as well as by comparing left ventricular area, taking conventional breath-hold Cartesian-cine (C-CINE) acquisition as reference.Purpose
To compare central k-space amplitude-only (ASG) vs. phase-only based SG (PSG) reconstructions in CMRI.Method
Two healthy adult volunteers underwent cardiac imaging on a 3.0T Siemens Verio scanner. First, C-CINE (FLASH) data was acquired with the following scanning parameters: TR/TE:50.4/2.42ms, flip angle: 15⁰, and voxel size: 2.2x1.8x8 mm3, Navg = 1. A spoiled gradient echo sequence with radial sampling scheme and Golden angle increments in spoke angles was implemented with the following scan parameters: TR/TE: 14/4.72ms, flip angle: 35⁰, Nr = 720, Np: 1005, dynamic repetitions: 12, and voxel size: 0.5x0.5x8 mm3, scan time: 2.3min/slice, Navg = 1. For easy reference, the sequence is dubbed GARAGE - for Golden Angle sampled Radial Gradient Echo. All the data was collected using a 6 channel flex coil along with a 4 channel spine coil. Data were acquired with 70% partial echo.Data Analysis
The central k-space magnitude profile and phase profile were acquired and Fourier transformed to evaluate their temporal frequency content. Using a notch filter, the respiratory and cardiac frequency components were then separated by taking signal peaks in the neighborhood of 0.25Hz and 1.25Hz respectively for PSG and ASG signals. The periodic signal (respiratory or cardiac) was then employed to identify the cardiac (or respiratory) cycle by detecting valleys of the function and the duration between two valley points representing one heartbeat/respiration. The GARAGE data was reconstructed into the same number of cardiac phases as the C-CINE image (25 phases - volunteer A, 13 phases – volunteer B). From the same datasets, two respiratory phases – inspiration and expiration, were reconstructed, for systole and diastolic cardiac phases using the SG approach.Results
Signal profiles from the amplitude and phase components of the k-space center from one coil, are plotted in Figure 1. Signal variation corresponding to respiratory motion as well as cardiac motion can be clearly visualized in both phase and amplitude. However, in another coil, only phase is seen to show consistent sensitivity to respiratory motion (Figure 2). Figure 3 shows the comparison of PSG and ASG reconstructions with the conventional C-CINE data for a 4-chamber view acquisition. The PSG and ASG reconstructions were both of comparable quality to the C-CINE data, but with higher spatial resolution. Figure 4 shows the inspiration and expiration PSG reconstructions of the heart in the short axis view, at systole and diastole. Figure 5 shows the relative volume changes of the left ventricle measured over the cardiac cycle from the PSG and ASG reconstructions and the C-CINE data. The volume-change curves are almost identical to one another confirming that ASG and PSG provide accurate and equivalent quality free-breathing reconstructions.Discussion and Conclusion
In this work, using explicit examples, we compared the efficacy of k-space center’s amplitude vs. phase based self-gating signal in reconstructing cardiac MRI images under free-breathing conditions. We found that both approaches can provide equal quality reconstructions when the signal amplitude is high. However, k-space center’s phase based self-gating signal provides an advantage when coil sensitivity profiles affect the amplitude sensitivity to motion. An approach where information from both the ASG and PSG data are combined may provide optimal self -triggering for imaging with free-breathing cardiac MRI.Acknowledgements
No acknowledgement found.References
1. Liu J, Spincemaille P, Codella NCF, et al, 2010. Respiratory and cardiac self-gated free-breathing cardiac CINE imaging with multiecho 3D hybrid radial SSFP acquisition. Magnetic resonance in medicine. 2010;63(5):1230-1237.
2. Feng L, Axel L, Chandarana H, et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magnetic resonance in medicine. 2016;75(2):775-788. 3. Larson AC, White RD, Laub G, et al. Self-gated cardiac cine MRI. Magnetic Resonance in Medicine. 2004;51(1):93-102.
4. Hiba B, Richard N, Janier M, et al. Cardiac and respiratory double self-gated cine MRI in the mouse at 7 T. Magnetic resonance in medicine. 2006;55(3):506-513.
Figures
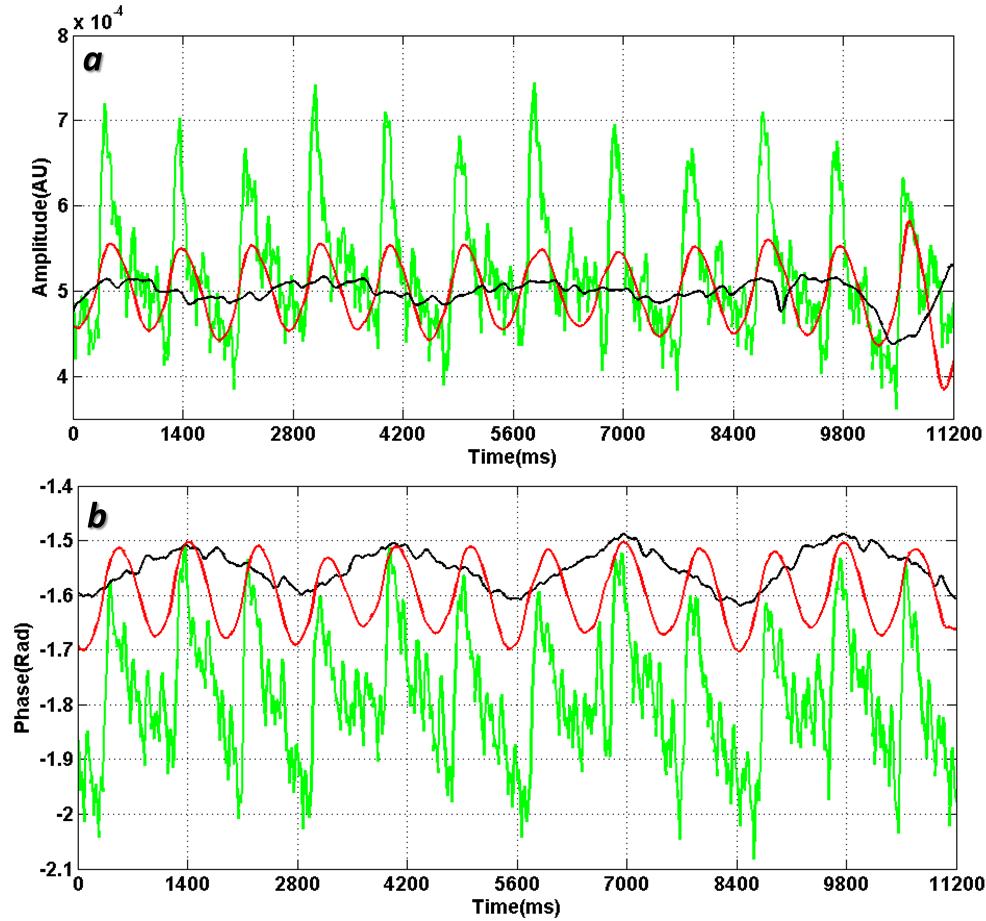
Figure-1. Self-Gating Signal (Volunteer A)
a.ASG . b. PSG
Green curves: central k-space signal.
Black curves: Respiratory self-gating signal
Red curves: Cardiac self-gating signal

Figure-2. ASG vs. PSG (Volunteer A)
Central k-space data: amplitude (blue), phase (cyan).
Respiratory self-gating: amplitude (red), phase (yellow).
Cardiac self-gating: amplitude (green), phase (purple).
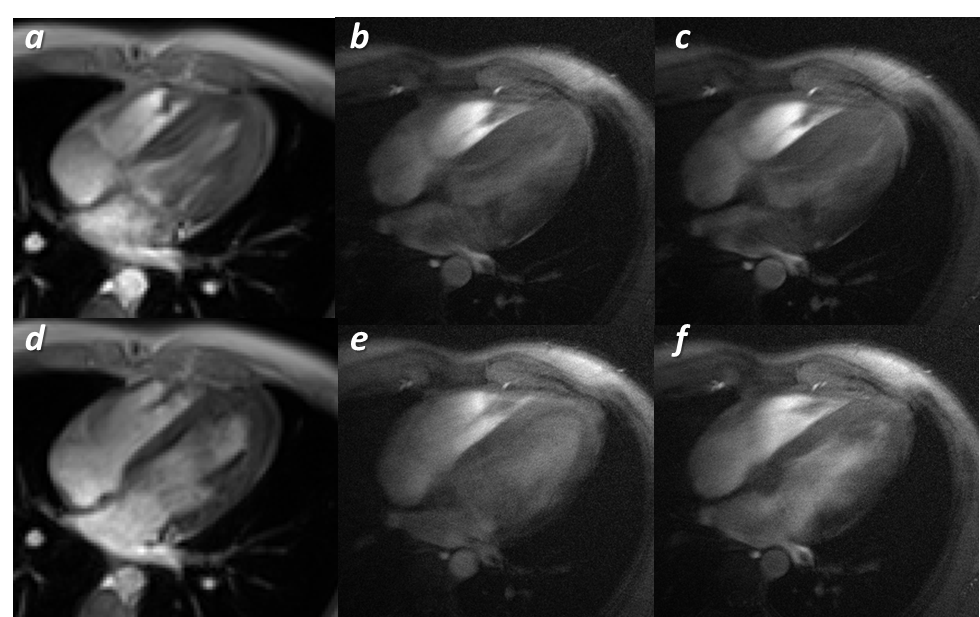
Figure-3. Four Chamber View Images (Volunteer B)
a. Systole (C-CINE MRI). b. Systole (ASG). c. Systole (PSG).
d. Diastole (C-CINE MRI). e. Diastole (ASG). f. Diastole(PSG).
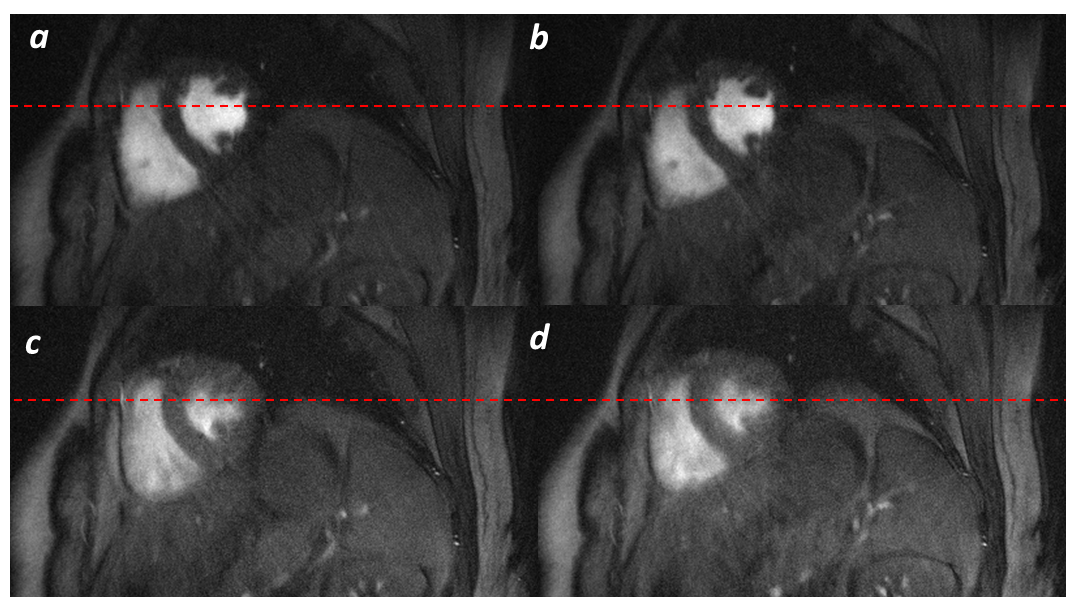
Figure-4. Cardiac Phase and Respiratory Phase (Volunteer A, PSG)
a.Cardiac phase one and respiratory phase one.
b.Cardiac phase one and respiratory phase two.
c.Cardiac phase two and respiratory phase one.
d.Cardiac phase two and respiratory phase two.
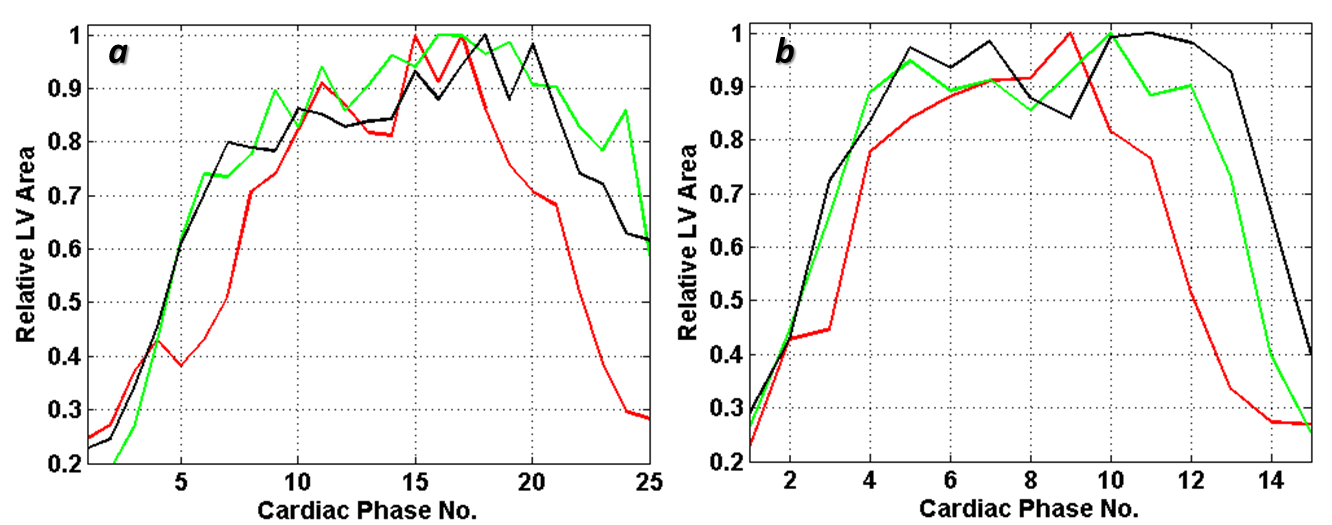
Figure-5. LV Area Variation
a.Volunteer A. b. Volunteer B.
Red Curve: CINE image. Green Curve: ASG. Black Curve: PSG.