4752
Optimized PC-MRA using a New Processing Workflow for 4D Flow MRI DataLingzi Tashakkor1, Susanne Schnell1, Alex J Barker1, Kelly Jarvis1, Emilie Bollache1, and Michael Markl1
1Northwestern University, Chicago, IL, United States
Synopsis
A new workflow was developed based on the information from 4D flow MRI to optimize the phase contrast MR angiogram. Five new PC-MRA algorithms were tested on 15 patients, and compared with and without the proposed pre-processing. Histogram equalization/remapping was applied to improve the dynamic signal range for easier segmentation and reduced user interaction. Results showed higher-quality PC-MRAs when the proposed pre-processing was applied.
Purpose
Magnetic resonance angiography (MRA) is widely used for diagnosing vascular diseases.1 As a potential
alternative, 4D flow MRI data (time-resolved 3D phase-contrast (PC) MRI with
3-directional velocity encoding) can be used to calculate 3D PC-MRA.1 3D PC-MRA data is used to depict anatomical features in combination with 3D blood flow
visualization, quantification of vessel dimension, or used as baseline data for the
3D segmentation of the vessel of interest.2 Moreover, 4D flow
derived 3D PC-MRA data does not require the injection of Gd-contrast media.2
However, existing 3D PC-MRA algorithms can have poor contrast or can insufficiently remove background signals, which can reduce image quality and hamper efficient 3D
segmentation. The goal of this study was to improve the quality of 3D PC-MRA
data by developing a new pipeline to pre-process the PC-MRA data. We systematically evaluated the new workflow
in a study with 15 subjects with 4D flow MRI of the thoracic aorta.Methods
Fifteen patients were included in our study: 5 healthy volunteers (age=41±10 years, 1 female) with 4D flow MRI after contrast agent administration, 5 healthy volunteers (age=49±10 years, 1 female) with non-contrast 4D flow MRI, and 5 patients with aortic valve stands (age=56±17 years, 0 female) with 4D flow MRI after contrast agent administration. All 4D flow MRI data were acquired using a 3T MR-System (Siemens MAGNETOM Skyra) with an ECG- and respiratory navigator gated time-resolved 3D PC Gradientecho sequence and 3-directional flow encoding (spatial resolution 3.2×2.22×2.63 mm3, temporal resolution=36.8-40 ms, TE=2.2-2.5 ms, TR=4.6-5 ms, venc=150-350).2 Fig.1A shows the 3D PC-MRA analysis workflow. First, the velocity standard deviation (STDEV) probability density function (PDF) masks were generated by calculating the STDEV of the absolute velocities for each velocity direction over time. The mean and STDEV for each set were used to define high, intermediate, and low STDEV regions. Probabilities were assigned to each voxel and then classified as vessels, tissue or noise. Second, a velocity mask was generated using information from time-averaged speed (TS) and peak systolic velocity (PS) to identify vessels. Information from TS and PS were combined to classify each voxel as vessel, tissue or noise, with probabilities being assigned accordingly. Third, k-mean clustering was used to classify and assign a probability for one of the categories. Finally, all three masks were combined to obtain a final PDF mask for weighting the PC-MRA calculations. Five PC-MRA algorithms were used (Fig.1B). Afterwards, histogram equalization/remapping was performed to improve the dynamic signal range of PC-MRA by remapping a 0.2% of the top intensities to a single, fixed point. Resulting PC-MRAs with and without pre-processing, as well as with histogram remapping were compared in regards of lumen-to-background contrast ratios (LBRs). One-tailed paired student t-test was performed between all subgroups to identify the best image quality workflow and algorithm (Table 1). To demonstrate the benefit of histogram equalization, the original PC-MRA data and histogram-equalized PC-MRA data were loaded into 3D segmentation software (Mimics, Materialise) and compared. Histogram-based thresholding was performed, followed by a seeded region grow to obtain the 3D segmentation of the aorta (Fig.4).Results
Comparing PC-MRAs with and without pre-processing shows that they benefit from the removal of noise and static tissue (Fig.2). Algorithms 1 and 3 produced a noticeable quality improvement in MIPs compared to the other algorithms. This finding agreed with the LBR in Fig.3. Since algorithm 3 does not use all the time information, algorithm 1 was used for histogram remapping. In Fig.2, pre-processed stenosis patient’s MIPs show rough edges and holes on the aorta. This is because stenosis patients' data features are different from the controls: the pre-processing algorithm may be suppressing false-positive voxels. Results from the paired t-test in Table 1 indicate that pre-processing can significantly improve LBRs. Fig.4 demonstrates that the equalized histogram has improved dynamic signal range. The histogram-equalized data was easier and more accurately segmented with less information loss and less user interaction.Discussion
A new method to extract the PC-MRA from 4D flow MRI data was explored. Static tissue and noise were identified and suppressed. Histogram equalization improved the dynamic signal range of the PC-MRA, thus allowing quick and accurate segmentation of vascular structures with minimal user interaction. The study indicates a robust, automated pre-processing work flow can be achieved with information provided by 4D flow MRI. Future work includes refining the calculation of masks and additional studies to compare 4D flow derived 3D PC-MRA data to the clinical reference standard contrast enhanced MRA.Acknowledgements
No acknowledgement found.References
1. Kriuluta AJ, González RG. Magnetic resonance angiography: physical principles and applications. Handb Clin Neurol. 2016;135:137-49.
2. Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4D flow MRI. J Magn Reson Imaging. 2012 Nov;36(5):1015-36.
Figures
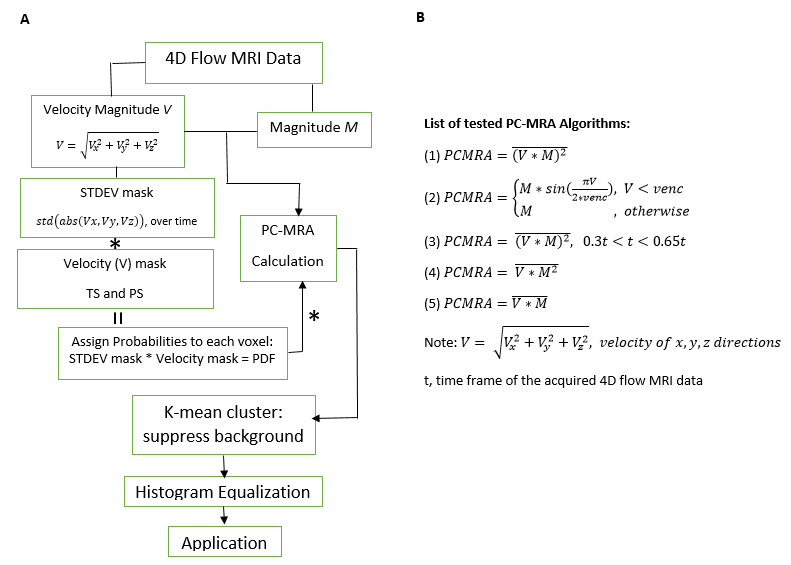
Fig.1. [A]
Data processing workflow. To identify noise and static tissue, a standard
deviation (STDEV) mask and velocity mask were generated and converted to a PDF.
The PDF is applied to the PC-MRA (calculated using each option shown in list B). K-mean clustering is performed to identify and delete background noise
from the PC-MRA. Histogram-equalization is shown to be useful for spreading signal
values evenly over the histogram spectrum.
[B] A list of tested PC-MRA algorithms.
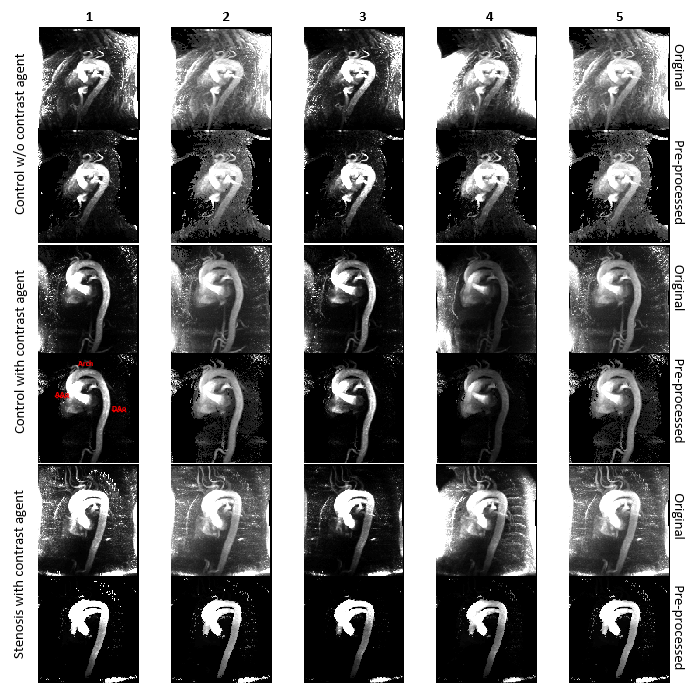
Fig.2. Comparison of 5 PC-MRA algorithms listed in Fig1B. Images are generated from the Maximum Intensity Projection (MIP). Three patients
are displayed: a control patient without contrast agent, a control patient with
contrast agent, and a stenosis patient with contrast agent administration.
For each patient, the top rows are the original non-preprocessed PCMRAs; the bottom rows
are the preprocessed PCMRAs.
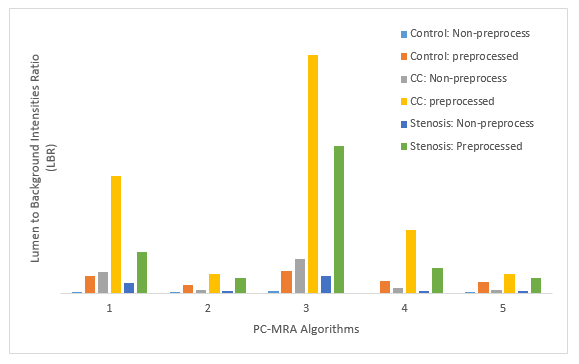
Fig.3. Image Contrast Quality Assessment. Fifteen patients’ data
were used to calculate PC-MRAs with and without pre-processing. Each set of
PC-MRAs’ LBRs are assessed. Control: 5 control without contrast agent patients’
data. CC: 5 control with contrast agent patients’ data. Stenosis: 5 stenosis
patients’ data.

Fig.4. Effect of histogram equalization: 3D (1)-PCMRA
aorta segmented in Mimics and its histogram plotted in Matlab. Left: Original
all data and original aorta data (without histogram equalization) plotted in
Matlab. Right: histogram equalized all data and aorta data plotted in Matlab. Segmentations
are performed in Mimics, with selected threshold (aiming for no holes on aorta),
followed by a seeded region grow with a seed on aorta.
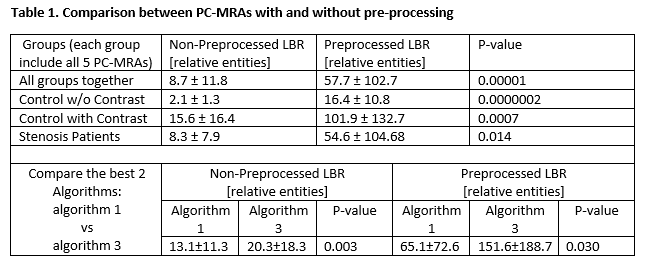
Table 1. Comparison between PC-MRAs with and without
pre-processing. One-tailed
paired student t-tests are performed to
compare
LBRs between subgroups (control without contrast agent, control with contrast agent,
and stenosis patients) and identify the workflow that results in
the best image quality (is significantly better, p<0.05, compared to others).
The test was also performed on algorithms 1 and 3 to prove
statistically that 3 is significantly better than 1, both with and without
pre-processing. However, algorithm 3 does not include all time frames.