4727
Arterial transit time measured by multi-delay ASL perfusion for evaluating major cerebral artery stenosis/occlusive disease: correlation with 15O-H2O and 15O2 gas PET-CBF and OEF1Department of Radiology, University of Fukui, Fukui, Japan, 2Department of Neurosurgery, University of Fukui, Fukui, Japan, 3Biomedical Imaging Center, University of Fukui, Fukui, Japan, 4GE Healthcare, Calgary, Canada
Synopsis
Positron emission computed tomography (PET) is used for evaluating cerebral hemodynamic ischemic stages in patients with major cerebrovascular stenosis/occlusion for treatment indication. Using a rapid, low-resolution pre-scan method, arterial transit time (ATT) and corrected cerebral blood flow (CBF) could be obtained, even in the immediate clinical setting. This study aimed to clarify whether ATT is hemodynamically related to misery perfusion stratified with 15O-H2O/15O2-gas PET data. There was a significant correlation between ASL and PET CBF before and after ATT correction (r2=0.27, 0.55). ATT also significantly correlated with PET-OEF (r2=0.11) and is a useful parameter to classify cerebral ischemia.
PURPOSE:
Brain
perfusion PET is widely used for evaluating major cerebral artery
stenosis/occlusive disease to determine whether treatment is indicated.
Patients are divided into cerebral hemodynamic ischemic state using the oxygen
extraction fraction (OEF) and CBF ratio
measured by PET1). Arterial spin labeling (ASL) also provides a means
of non-invasive assessment of brain perfusion on MRI. Previous reports have
shown prolonged ATT2) and correlation between the metrics from positron
emission tomography and ASL in patients with major cerebral artery occlusive
disease, suggesting the possibility that ATT can also assess hemodynamic
cerebral ischemia3,4). Single post-labeling delay (PLD) ASL may
cause underestimation due to errors associated with fixed ATT assumption when ASL
perfusion is applied to patients with major vessel stenosis/occlusive disease.
Therefore, multiple PLD ASL acquisitions
and ATTs are necessary to obtain correct CBF values. Reduced resolution ATT pre-scan has been proposed for ATT-corrected
ASL perfusion imaging with the short scan time method5), which may
be feasible for patients within a clinically acceptable time for assessment of
both ATT and ATT-corrected CBF.
Thus, we
sought to clarify whether ATT is hemodynamically related to the misery
perfusion state classified with PET CBF data.
MATERIALS AND METHODS:
Nine patients (6 men [median age, 68.5 years;
range, 57-73 years] and 3 women [median age, 45 years; range, 43-69 years])
with cerebrovascular stenosis/occlusive disease underwent ASL and PET at least
1 month after a symptomatic event such as hemiparesis with dysarthria. MRI was
performed using a 3.0-T whole-body scanner (Discovery MR 750; GE Healthcare,
Waukesha, WI, USA) and 32-channel head coil. The patients were examined using pseudo-continuous
ASL pulse sequence and 3D spin echo spiral readout with vessel suppression
gradient. Imaging parameters were as follows: labeling pulse duration, 4.0 s;
PLD 2.0 s; TR 7502.2 ms; TE 22.6 ms; spiral acquisition (512 points × 7 arms); FOV
240×240 mm; 38 to 40 slices covering the whole brain. We measured ATT
using a low-resolution (640 × 2 arms) pre-scan approach with 5 PLD,
0.70/1.26/1.85/2.43/3.0 s, based on the previously reported methods5).
Then, PET
CBF was performed using
the dual-table autoradiography method. Eight regions of
interest (ROIs) (4 for each hemisphere) at the bilateral anterior cerebral
artery and anterior/posterior middle
cerebral artery territories and
posterior cerebral artery were analyzed, which were automatically detected with
NEURO FLEXER (Nihon Medi-Physics Co., Ltd, Tokyo, Japan) for objective
analysis. Before using NEURO FLEXER, an ATT map was scaled using a brain mask image
made from proton images. ATT measured by ASL and CBF/OEF measured by PET were
used for linear regression analysis. Each ROI was labeled into hemodynamic
ischemic stages using the data of CBF/OEF
measured by PET; ATTs in each ROI were compared using the Scheffe multiple
comparison procedure.
Fig. 1 shows a representative case.
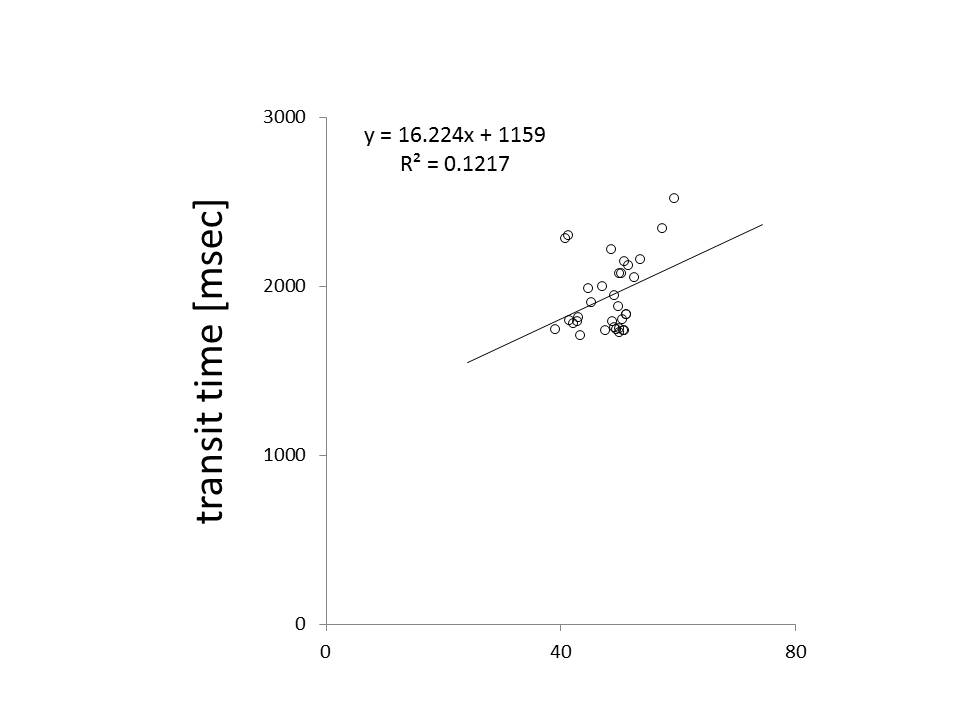
The correlation between PET and ASL-CBF were r=0.72 in all ROIs with the correction of ATT. A significant linear correlation existed between ATT and OEF (r2=0.1746, p<0.025) in ROIs with longer ATT than 1700ms, while overall ROIs ATT have no such significant correlation.
This study demonstrates a significant correlation between ASL and PET-CBF. Moreover, ATT could detect ischemic state area using a cut-off value of 1700 ms in a cohort of 9 patients with major cerebral artery stenosis/occlusion. It would be clinically useful to use ATT to detect misery perfusion because patients could avoid acetazolamide injection, which has recently been reported to have adverse effects in some cases by an unknown mechanism.
The brain has an autoregulatory function to maintain cerebral blood flow. In the state of reduced cerebral perfusion pressure due to chronic major cerebral artery stenosis/occlusion, the arteriolar cerebral vessels dilate, which may cause the decline of cerebral perfusion resistance and hence prolonged mean transit time. ATT is hypothetically affected not only by the time delay while passing collateral circulation but also the time delay caused by misery perfusion and the autoregulatory response noted above, and we suggest that this is the possible reason why ATT could reflect hemodynamic cerebrovascular ischemia.
ATT is a useful parameter for evaluating patients with major cerebral artery stenosis or occlusive disease to detect misery perfusion area, and CBF corrected by ATT is more precise than without correction.
Acknowledgements
No acknowledgement found.References
1) Nakagawara J. No To Shinkei. 1999;51(6):502-13.2) Bokkers RP, et al. Am
J Neuroradiol. 2008;29(9):1698-703
3) Kimura H,
et al. Proceedings of ISMRM 2009: 3646.
4) Kamano H, et al. Acta Radiol 2012;54(1)99-106
5) Dai W, et al.
Magn Reson Med. 2012;67(5):1252-65
Figures
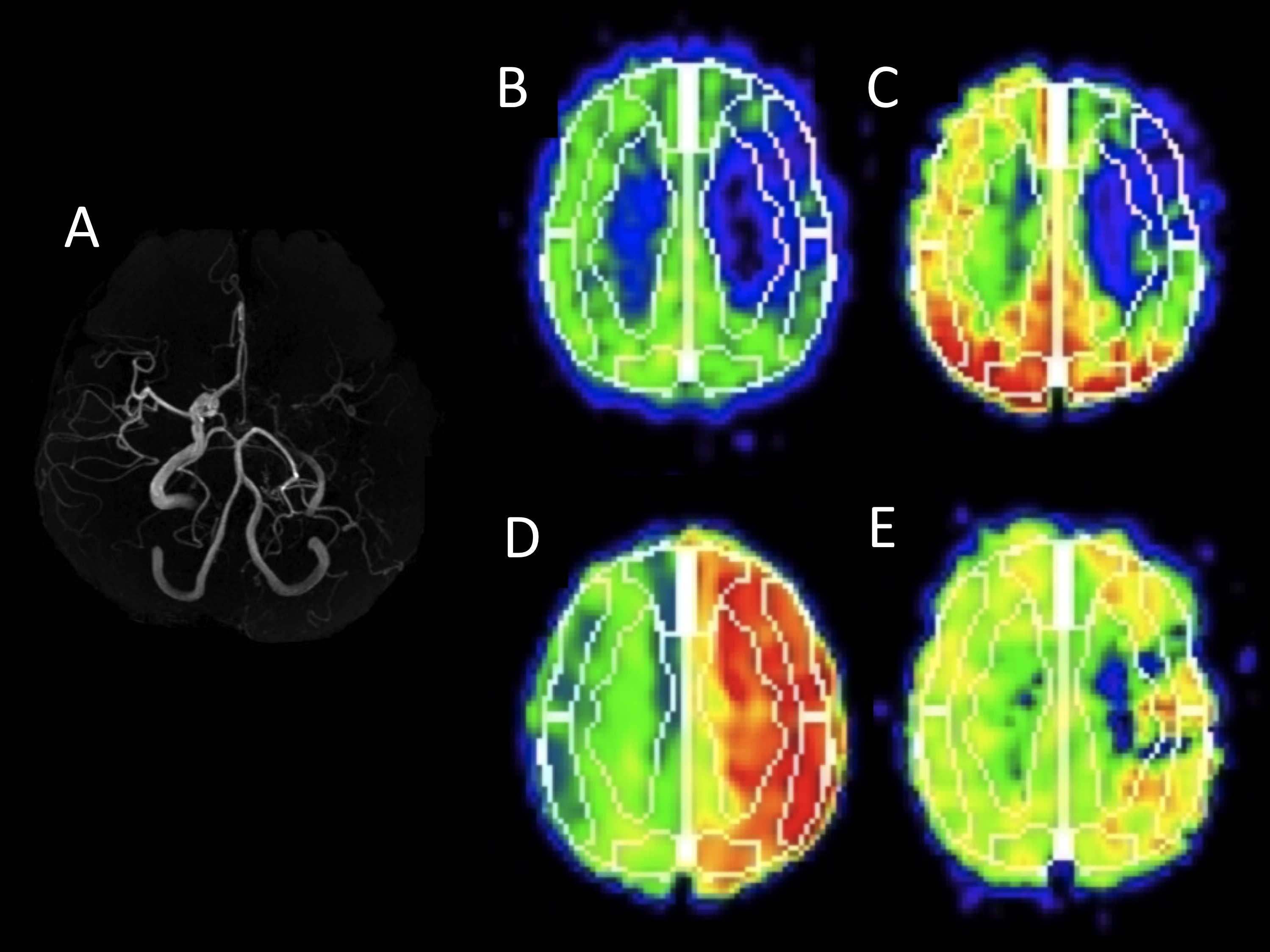
Figure 1. A representative image of a 71-year-old man with chronic internal carotid artery occlusion
A)Magnetic resonance angiography maximum intensity projection, B) transit time map, C) transit time corrected cerebral blood flow(CBF), D) PET-CBF, E)oxygen extraction fraction(OEF)
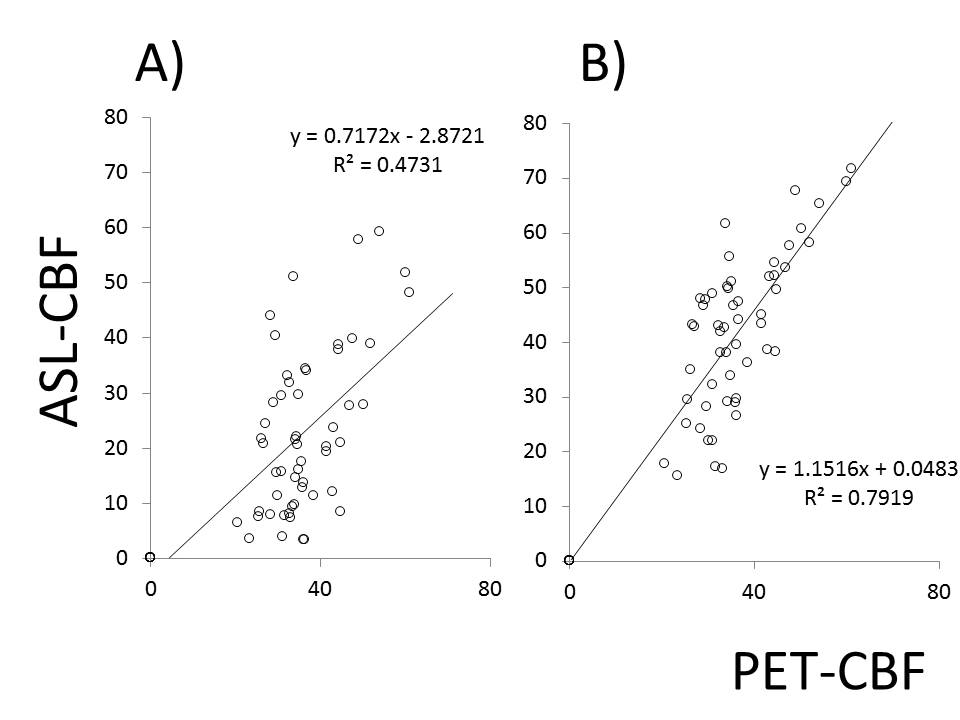
Figure 2. Comparison
between ASL-CBF and PET-CBF.
A) labeling
pulse duration, 4.0 s; PLD 0.7 s.
B) labeling
pulse duration, 4.0 s; PLD 2.0 s. CBF corrected by ATT.