4710
Intramural Hematoma Detection by Susceptibility-weighted Angiography (SWAN) in Intracranial Vertebral Artery DissectionHideki Ishimaru1, Minoru Morikawa1, Reiko Ideguchi1, Yohei Ikebe1, and Masataka Uetani1
1Radiology, Nagasaki University Hospital, Nagasaki, Japan
Synopsis
Vessel wall susceptibility on SWAN with no calcification on CT indicates intramural hematoma (IMH) associated with vertebral artery dissection (VAD). The early detection of IMH in VAD can be enhanced with the use of SWAN.
Introduction
Intramural hematoma (IMH), a pathognomonic feature of arterial dissection, is hardly distinguishable from atherosclerotic plaque in the acute stage because both show intermediate signal on T1-weighted imaging, however, the early detection of IMH can be enhanced with the use of susceptibility weighted imaging1. Susceptibility-weighted angiography (SWAN), which uses multiple magnitude images with different echo times for the image generation, is highly sensitive to both paramagnetic and diamagnetic compounds2; it is therefore hypothesized that SWAN can be sensitive in delineation of IMH by susceptibility effect in the vessel wall. The purpose of the study was to evaluate the diagnostic accuracy of SWAN in intracranial vertebral artery dissection (VAD).Methods
The lesions in the cohort included 33 intracranial vertebral artery lesions: 16 non-hemorrhagic VADs (50%) confirmed by double lumen on catheter angiography (n=8) or chronological shrinkage of T1-hyperintense IMH (n=8), and 16 atherosclerotic lesions (50%) as a control group. Images were taken using 3.0 T or 1.5T MR system (Signa HDxt, GE) using an 8-channel head coil. SWAN acquisition was performed using three dimensional (3D) multi-echo gradient echo sequence with following parameters: FA = 15, TR = 31 ms, 5 TEs centered around 23 ms, matrix size = 324 × 224, FOV = 27.8 × 20 cm and slice thickness = 2.4 mm on a 3T scanner and FA = 15, TR = 64 ms, 5 TEs centered around 50 ms, matrix size = 384 × 192, FOV = 30 × 22 cm and slice thickness = 3 mm on a 1.5T scanner. TOF-MRA were taken in all patients. High-resolution T1 - and T2 -weighted MRI (plaque images) were taken in case-by-case patients. Two experienced neuroradiologists collaboratively and retrospectively evaluated the presence of eccentric or concentric dark signal (vessel wall susceptibility) at the distal vertebral arterial wall on SWAN images. Brain CTs were also evaluated to see the presence or absence of vessel wall calcification in the corresponding areas of susceptibility, because calcification can be another cause of susceptibility. Statistical analysis was done to evaluate the sensitivity and specificity of the vessel wall susceptibility on SWAN for the diagnosis of VAD. Two-by-two contingency tables were made and analyzed by means of the Fisher exact test.Results
Vessel wall susceptibility was positive in all 16 cases of VAD and in 12 out of the 16 cases of the atherosclerosis. It showed a sensitivity of 100% and specificity of 25% for the diagnosis of VAD (P = 0.10). The vessel wall susceptibility was correlated with the corresponding area of T1-hyperintense IMH in 8 cases of VAD. Corresponding vessel wall calcification was obvious in none of 16 cases of VAD and 10 of 12 positive cases of atherosclerosis. When susceptibility without vessel wall calcification was considered as positive IMH sign, specificity was increased up to 87.5% (Fig 3). In 3 VAD cases followed by SWAN, vessel wall susceptibility decreased in a few months, corresponding to shrinkage of IMH on plaque imaging (Fig 1).Discussion
SWAN is a weighted sum of the images obtained at different TEs and results in heavily susceptibility weighted images. Combining the information of these multiple TEs with a first TE using the arterial inflow (time of flight) effect a simultaneous visualization of both cerebral arteries and susceptible components (e.g., hemosiderin, calcification) is possible. It facilitates detection of vessel wall susceptibility as dark signal around bright signal of arterial lumen. That is a reason why SWAN showed a sensitivity of 100% for the diagnosis of VAD. A disadvantage of the SWAN is that hemosiderin cannot be distinguished from calcification; for this reason we evaluated brain CT to exclude vessel wall susceptibility due to calcification. Thus, IMH sign on SWAN achieved a sensitivity of 100% at a specificity of 87.5% for the diagnosis of VAD. A drawback of this study is that we used a relatively small and limited sample consisting of VAD and vertebral artery atherosclerosis. SWAN sequence that we used has problems in visualizing peripheral arteries and arteries near skull base due to relatively low slice resolution and blooming artifact of the skull base . Improvement of imaging parameters, such as the thinner slice thickness and shorter TE, is needed.Conclusion
IMH sign on SWAN (vessel wall susceptibility with no calcification on CT) was significantly associated with VAD. The detection of IMH in VAD can be enhanced with the use of SWAN; however, the brain CT is necessary to exclude vessel wall calcification due to atherosclerosis.Acknowledgements
No acknowledgement found.References
1. Kim TW, Choi HS, Koo J, et al. Intramural hematoma detection by susceptibility-weighted imaging in intracranial vertebral artery dissection. Cerebrovasc Dis. 2013;36: 292-298.
2. Boeckh-Behrens T, Lutz J, Lummel N, et al. Susceptibility-weighted angiography (SWAN) of cerebral veins and arteries compared to TOF-MRA. Eur J Radiol. 2012;81: 1238-1245.
Figures
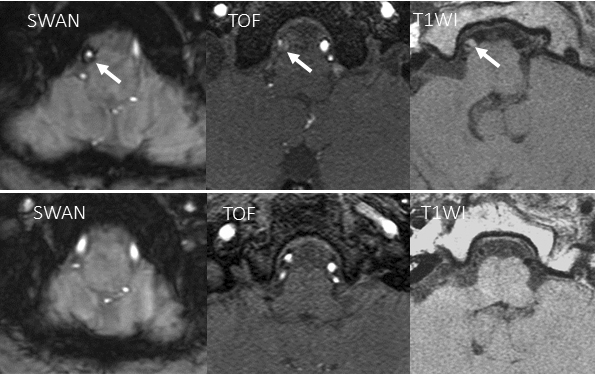
Fig.1 Representative case for
defining vessel wall susceptibility on SWAN in vertebral artery dissection (top).
Concentric dark signal in right distal vertebral arterial wall on SWAN with
corresponding double lumen on TOF and T1 hyperintense intramural hematoma (IMH)
on T1WI. A follow up study obtained
three months later (bottom) shows shrinkage of vessel wall susceptibility on SWAN
and IMH on T1WI.
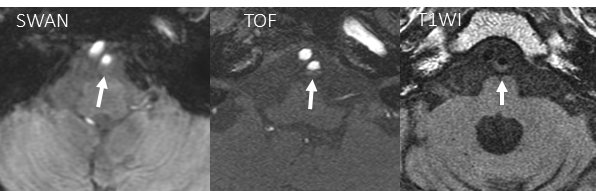
Fig.2 Representative case of
atherosclerosis. T1WI shows eccentric wall thickening of left vertebral artery
(VA). No corresponding dark signal in
left VA on SWAN.
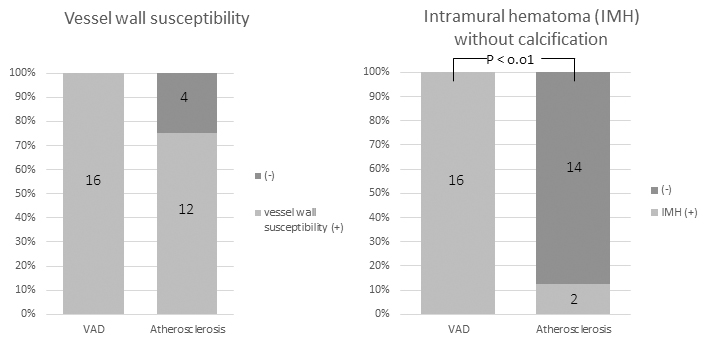
Fig.3 Comparison of vessel
wall susceptibility (left) and intramural hematoma (right) in patients with VAD
and atherosclerosis.