4707
ICA-based overt speech artifact removal leads to improved estimation of deconvolution-based hemodynamic response function in aphasics1Dept. of Neurology, Emory University, Atlanta, GA, United States, 2Center for Visual and Neurocognitive Rehabilitation, Atlanta VAMC, Decatur, GA, United States, 3Dept. of Physics & Astronomy, Georgia State University, Atlanta, GA, United States, 4University of Florida, Gainesville, FL, United States, 5Dept. of Radiology & Imaging Sciences, Emory University, Atlanta, GA, United States, 6Dept. of Psychology, Georgia State University, Atlanta, United States
Synopsis
Overt speech task functional Magnetic Resonance Imaging (fMRI) paradigms are very attractive to study aphasic patients, but are also plagued by task-correlated motion (TCM). Speech involves movements of the mouth and soft palate, and causes a change in air volume around these areas leading to localized motion and susceptibility artifacts. These artifacts become more severe in patients with Aphasia. The goal of this study is to utilize existing FSL-based semi-automated ICA tools, and optimize them to go beyond removing standard fMRI artifacts by also mitigating TCM artifacts to obtain meaningful hemodynamic response function (HRF) in aphasic patients. Our preliminary results to utilize ICA for TCM-based artifact removal is promising as evidenced by the improved sensitivity and specificity, but needs further optimization. Optimal denoising of overt speech task fMRI in aphasic patients will also help us to delineate their task-based networks in an effort to monitor plastic changes due to language behavior interventions.
Purpose
Overt speech task functional Magnetic Resonance Imaging (fMRI) paradigms are very attractive to study aphasic patients, but are also plagued by task-correlated motion (TCM). Speech involves movements of the mouth and soft palate, and causes a change in air volume around these areas leading to localized motion and susceptibility artifacts. These artifacts become more severe in patients with Aphasia. Several studies1-4 have developed clever methodologies to overcome TCM artifacts, but we still lack a relatively easy and computationally time-efficient technique that maintains the specificity-sensitivity balance in detection of task-related functional activity. Independent Component Analysis (ICA) is able to decompose fMRI time series into non-co-linear spatial maps and time series4 which has been further developed into semi-automated software packages to identify and remove standard fMRI artifacts5-6. The goal of this study is to utilize existing FSL-based semi-automated ICA tools, and optimize them to go beyond removing standard fMRI artifacts by also mitigating TCM artifacts to obtain meaningful hemodynamic response function (HRF) in aphasic patients.Methods
Subjects: We recruited nine monolingual English speaking post-stroke patients (mean age=68) with aphasia (>6months). MRI: High-resolution T1-weighted MPRAGE structural images and six task-fMRI runs (sagittal acquisition, voxel=3.75x3.75x4mm3, 36slices, TR=1.7sec, no gap in TR, TE=30ms, FA=70°) were acquired on a Philips 3T Achieva using a 8-ch headcoil. During the task-fMRI runs, the patients heard and read a semantic category and attempted to overtly generate an exemplar of that category. fMRI pre-processing: The functional images were corrected for slice timing, global head motion, and coregistered to MPRAGE using Freesurfer boundary-based-registration algorithm. ICA-denoising: The pre-processed images were decomposed into temporal and spatial components using FSL MELODIC. We utilized 10 MELODIC outputs from different subjects to train the classifier algorithm via hand-labeling of “noisy” components using two stringency thresholds. The less stringent threshold incorporated: (a)stimulus-driven periodicity in time series, (b)high power-spectral density (PSD) at task frequency, and (c)assessing the HRF of ambiguous ICA time-component using deconvolution. The more stringent criteria were layered on top of the less stringent criteria: (i)accurate identification of aliased cardiac and respiratory frequencies, (ii)stringent spatial maps (e.g. exclude draining vein activity, retaining peri-lesional focused activity) and (iii)further exclusion of components with sharp and rapid fluctuations at stim onset (1-2TR changes) within the time-component. The hand-labeled datasets were fed to FSL FIX to obtain ‘trained’ classifiers, which was applied to the remaining datasets. The noise components were filtered (regfilt) from each run in a non-aggressive fashion. fMRI post-processing: The data sets were processed in 3 ways: no application of ICA (no ICA), less stringent ICA denoising, and more stringent ICA denoising. Each dataset was spatially smoothed (FWHM=6mm), and deconvolved with the task stimuli to generate a HRF (modeled with 11 tents) and statistical parametric activation map thresholded at R2=0.12 7 (corrected p=8e-22, cluster size>=20).Results
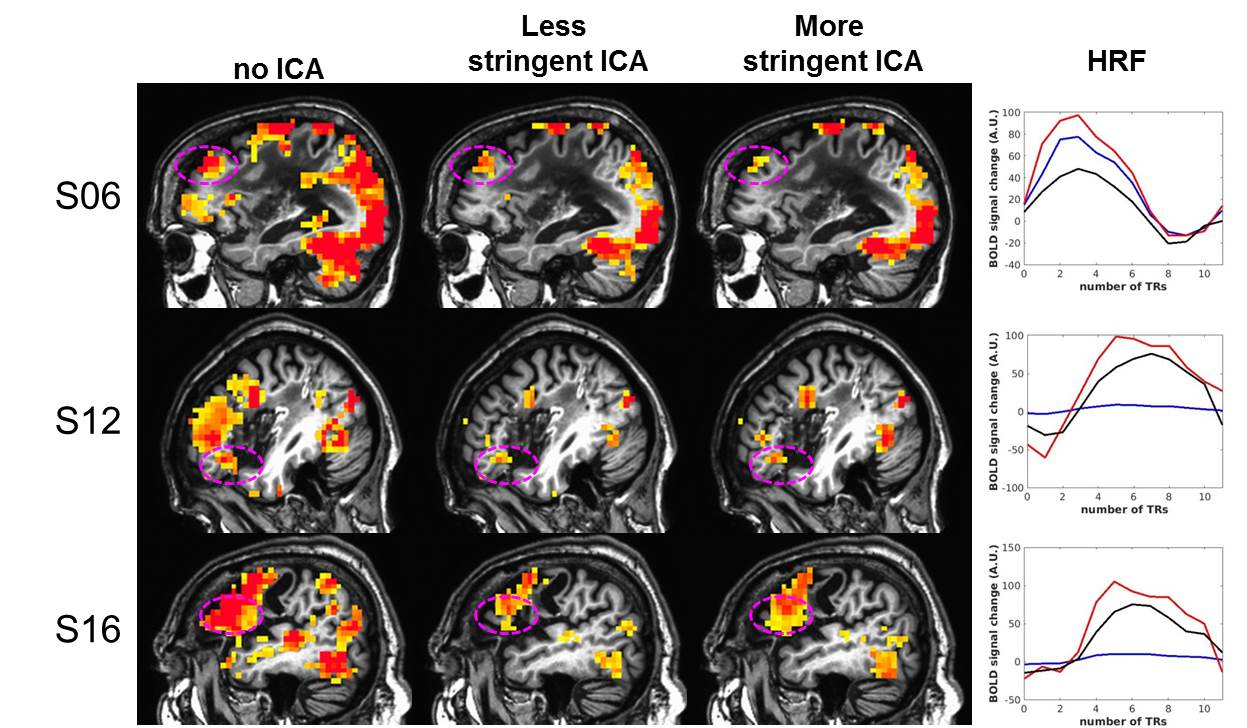
Across all 9 subjects, ICA denoising improves the specificity by removing false positive activation in ventricles, lesion, and TCM areas. The range of R2 across subjects was: no ICA=0.35-0.82; less stringent ICA=0.12-0.59; more stringent ICA=0.07-0.51, indicating that ICA denoising may lead to reduced sensitivity in some subjects. Six out of the 9 subjects survived the R2 threshold that were used to examine the HRFs. Figure 1 shows that the most stringent ICA not only increased the specificity in typical TCM plagued areas (such as temporal, medial and lateral frontal areas), but also increased the sensitivity to task-induced BOLD activation, particularly in Broca’s areas. From the sample subjects in Figure 1, we observe that most stringent ICA-corrected HRF does not have the rapid and sharp initial rise in BOLD (S06), and the shape of the BOLD HRF looks closer to ideal and expected HRF in stroke patients. In patients S12 and S16, most stringent ICA pulls the task-related BOLD signal out of the TCM noise bed that can be seen in no ICA, but in patient S06, the sensitivity to BOLD amplitude decreases with most stringent ICA.Discussion and Conclusion
Our preliminary results to utilize ICA for TCM-based artifact removal is promising as evidenced by the improved sensitivity and specificity, but needs further optimization. The advantage of FSL-based semi-automated ICA denoising tools is that it requires a one-time front-end effort to hand label and train the classifiers for specific dataset (depending on type of task and patient group) without the burden of excessive computational and labor time to denoise each dataset. Optimal denoising of overt speech task fMRI in aphasic patients will also help us to delineate their task-based networks in an effort to monitor plastic changes due to language behavior interventions.Acknowledgements
No acknowledgement found.References
[1] Gopinath K et.al Human Brain Mapp. 2009. [2] Kemeny S et.al Human Brain Mapp. 2005 [3] Peck KK et.al Stroke 2004. [4] McKeown MJ & Sejnowki TJ. Hum Brain Mapp 1998. [5] Smith SM et.al Neuroimage 2004 [6] Salimi-Khorshidi G et.al Neuroimage 2014. [7] Benjamin ML et.al Neurorehabil. Neural Repair 2014.Figures