4705
Evaluation of collaterals: comparison between cerebral perfusion using 3D TASL and FVH in unilateral internal carotid artery stenosis1Radiology, Chinese PLA general hospital, Beijing, People's Republic of China, 2Radiology, First affiliated hospital of Chinese PLA general hospital, Beijing, People's Republic of China
Synopsis
As a critical result in different researches the sign of FHV refers to the hemodynamic impairment and slow retrograde flow in leptomeningeal collaterals with or without good clinical outcome. We collected MR imaging data of 32 patients with unilateral ICA stenosis-occlusion who all underwent MR examinations by using 3D tASL perfusion imaging and T2-FLAIR. The tASL perfusion scores were compared between in FVH(-) group (14 patients) and FVH(+) group (18 patients), and there was no difference in the 2 groups. The result showed that 3D tASL perfusion MRI may be a useful non-invasive tool to identify the collateral flow.
PURPOSE
The fluid-attenuated inversion recovery vascular hyperintensities(FVH) as a useful sign which is frequently observed near the cerebral surface along the cortical sulci in patients with ischemic stroke respond to the hemodynamic impairment and slow retrograde flow in leptomeningeal collaterals[1]. Some studies indicated that FVH was an indicator of adequate collateral with good clinical outcomes [2], but other authors suggested that FVH were associated with large vessel occlusion or severe stenosis with insufficient collateralization [3]. The purpose of this study was to explore whether FHV is a useful tool to identify the adequate collaterals in patients with unilateral internal carotid artery (ICA) severe stenosis-occlusion by comparing the cerebral blood flow (CBF) map using 3D-territorial arterial spin labeling (3D tASL).METHODS
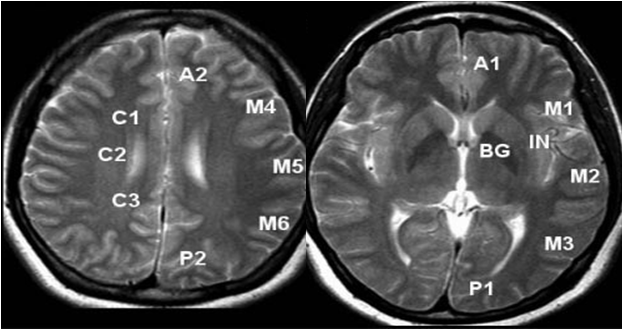
This retrospective study enrolled 32 consecutive patients(male 27, 84.4%)with unilateral ICA severe stenosis-occlusion (70%-100%) from August 2015 to July 2016 who underwent MRI scanning(the degrees of the stenosis of the ICA were identified by Intra-arterial digital subtraction angiography(DSA) before or after MRI scanning). The T2-FLAIR images and the perfusion data were separately obtained using T2-FLAIR sequence and 3D tASL sequences on 3.0-T MR scanner (Discovery 750, GE Medical Systems). According to the appearance of the FVH on T2-Flair images, the 32 patients were divided into two groups: FVH positive as FVH(-) and FVH negative as FVH(+). The perfusion data were evaluated and scored using a grading system similar to Kim[4]at 13 anatomic sites based on regional vascular territories(figure 1), manual drawing the region of CBF on GE ADW 4.5 workstation : the adequate collateral circulation as the CBF≥10 ml/min/100gas 1, and deficient CBF as CBF<10 ml/min/100g as 0. The range of the every patient score is 0-13. The tASL scores were compared between FVH (-) group and FVH (+) group.RESULTS
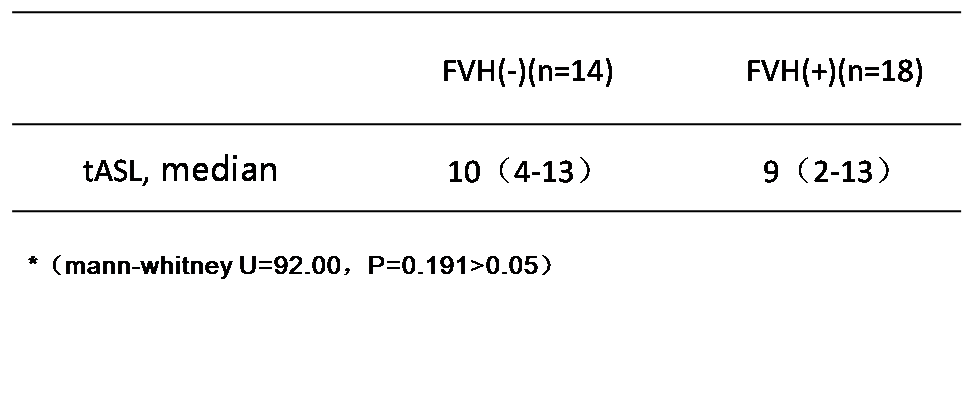
The FVH(-) group contained 14 patients and the median tASL score(median) was 10(4-13). The FVH(+) group contained 18 patients and the median tASL score(median) was 9(2-13). No significantly difference between the groups FVH(-) and FVH(+) with tASL score(mann-whitney U=92.00,P=0.191>0.05)(table.).CONCLUSION
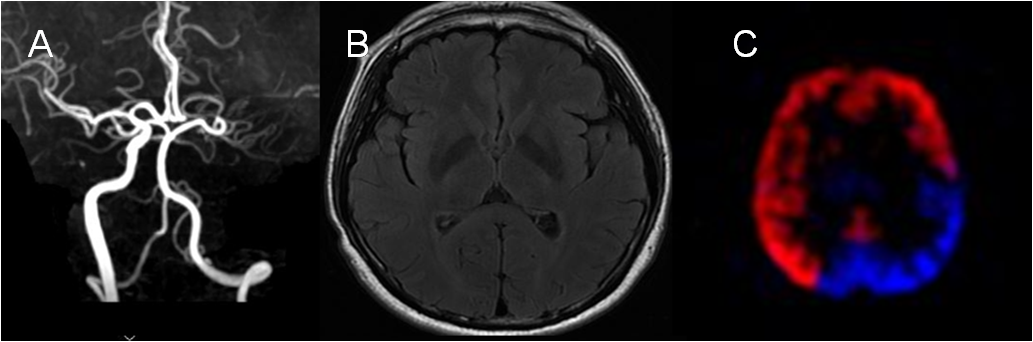
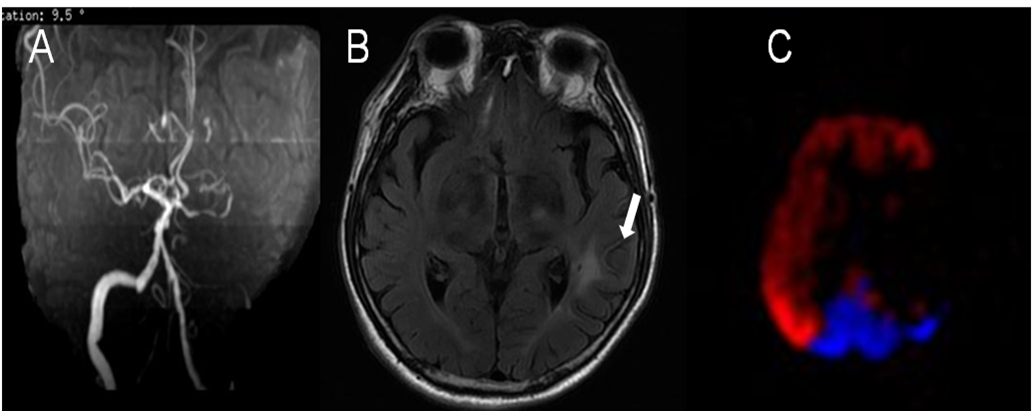
The collateral circulation status cannot be evaluated using FVH sufficiently, but it could be evaluated by 3D tASL perfusion directivity, which is performed in patients with ICA steno-occlusion (figure 2 and 3). The study has indicated that FVH may refer to the slow retrograde flow, not correlation with collateral. 3D tASL perfusion MRI may be a useful non-invasive tool to identify the presence, the origin, and distal function of collateral flow.Acknowledgements
No acknowledgement found.References
1. Cheng B, et al. Stroke. 2012;43:2957–2961.
2. Lee KY, et al. Neurology 2009;72:1134–39.
3. Kufner A, et al. AJNR Am J Neuroradiol. 2015;36:1426-30.
4. Jane J. Kim, et al. Stroke. 2004;35:1340-1344.
Figures