4673
Simple Modification of Arms Position Improves B1+ and Signal Homogeneity in the Thoracolumbar Spine at 3T1Department of Radiological Technology, Hokkaido University Hospital, Sapporo, Japan, 2Division of Diagnostic and Interventional Radiology, Hokkaido University Hospital, Sapporo, Japan, 3Hitachi, Ltd., Healthcare Company, 4Hitachi, Ltd., Research and Development Group
Synopsis
To evaluate the homogeneity of B1+ and signal intensity of the thoracolumbar spine with different arm positions. Twenty volunteers were scanned with 4-channel RF transmit coil at 3T. Three arm positions were used; arms on the bed, arm lift, and arm up position. Axial B1+ maps and sagittal T1WI were obtained individually with each arm position. Mean and SD values of FA, and CNR with arm lift and arm up position were significantly superior with arms on the bed position. Inhomogeneities of B1+ and signal intensities were improved by simply changing the arm position at 3T thoracolumbar spine imaging.
PURPOSE
Three-tesla (3T) magnetic resonance imaging (MRI) is more sensitive to radiofrequency magnetic field (B1+) inhomogeneities due to the standing effect of radiofrequency (RF) wave accentuated by shorter wavelength of RF, compared to 1.5T. These B1+ inhomogeneities have been reported especially at the thoracolumbar spinal imaging.1 Murbach et al. reported that the arms were one of the hotspot locations of local specific absorption rate (SAR) and temperature, using two-port body transmission coil in 3T abdominal imaging.2 The purpose of this study was to evaluate the homogeneity of B1+ and signal intensity with different arm positions at 3T thoracolumbar spinal imaging.METHODS
This study prospectively included 20 healthy volunteers. All MR imaging was performed with a whole-body 3T system (TRILLIUM OVAL; Hitachi, Ltd.) equipped with 4-channel RF transmit coil. During the scans, three types of arm positions were used; arms on the bed (conventional position), elevation of arms by 100mm (arm lift position) and elevation of arms above the shoulder (arm up position) (Fig.1). Axial B1+ maps at Th12, L3 and S1 level were obtained individually with each arm position. Short TR, small flip angle gradient echo sequence, reported as rapid B1+ mapping using phase-difference method, was used for the creation of B1+ maps.3. After obtaining B1+ maps, RF shimming was performed to achieve uniform B1+ transmission at whole scan range by using the three sectional B1+ maps. Sagittal T1WI was also obtained with each arm position. Scan range included from the vertebral level of Th10 to S3. ROI measurement of B1+ map was conducted with a rectangular ROI (150 × 120 mm) placed at center of vertebra on each B1+ map (vertebral levels of Th12 , L3, and S1). Freehand ROIs were placed on the spinal cord and cerebrospinal fluid (CSF) of sagittal T1WI. Contrast noise ratios (CNRs) between spinal cord and CSF were calculated and compared among three different arm positions. The mean and standard deviation (SD) of FA and CNR in the ROIs were calculated and compared among three different arm positions using one-way analysis of variance (ANOVA). The post-hoc Tukey tests were used to determine which pair of arms positions had a significant difference in the mean and SD of FA and CNR. The alpha level was set at 0.05.RESULTS
Mean FA values (degrees) with arm lift and arm up position (70.7±4.2 and 72.2±4.3, respectively at the Th12 level, 77.5±3.7 and 78.9±3.2, respectively at the L3 level, 76.4±3.4 and 78.0±3.4, respectively at the S1 level) were significantly larger than with conventional position (63.8±6.4 at the Th12, 72.2±5.6 at the L3, and 73.0±4.2 at the S1 level, respectively) (Fig.2). SD values of FA with arm lift and arm up position (0.139±0.044 and 0.143±0.035, respectively at the Th12 level, 0.097±0.018 and 0.100±0.016, respectively at the L3 level, 0.106±0.010 and 0.105±0.018, respectively at the S1 level) were significantly smaller than with conventional position (0.211±0.055 at the Th12, 0.137±0.044 at the L3, and 0.129±0.022 at the S1 level, respectively). CNR with arm lift and arm up position (3.26±0.95 and 3.39±1.00, respectively) were significantly higher than with conventional position (2.15±1.35) (Fig.3). There was no significant difference between arm lift position and arm up position in the all results.DISCUSSION
We observed the improvement of inhomogeneities in B1+ and signal intensity in arm lift and arm up position, which were possibly due to the reduction of RF interference by changing the arms position near the body trunk (Fig. 4 and 5).We considered that one of the reasons was the change in the symmetry of the body shape including arms. In the conventional position, the body shape including arms has only lateral symmetry. In the arm lift and arm up positions, the body shape has lateral and vertical symmetry. Therefore, the improvement of B1+ homogeneity in arm lift and arm up positions was due to the improvement in the symmetry of the body shape.CONCLUSION
Inhomogeneities of B1+ and signal intensities were improved by simply changing the arm position at 3T thoracolumbar spinal imaging. Both arm lift and arm up positions were effective; however, arm lift position has the advantage as it seems to be more comfortable for the patients especially for long examination time.Acknowledgements
The author is thankful for B1+ map analysis of Kousuke Itou, Hitachi Ltd.References
1. Bouvier J, Tropres I, Lamalle L, et al. Evaluation of dual-source parallel RF excitation technology in MRI of thoraco-lumbar spine at 3.0 T. J Neuroradiol. 2013;40(2):94-100.
2. Murbach M, Neufeld E, Cabot E, et al. Virtual population-based assessment of the impact of 3 Tesla radiofrequency shimming and thermoregulation on safety and B1+ uniformity. Magn Reson Med 2015.
3. Ito K, Takizawa M, Takahashi T. Rapid B1+ mapping method for multi-channel RF transmit coil using phase-difference. In: Proceedings of the 21st Annual Meeting of ISMRM, Salt Lake City, 2013. (abstract 2598).
Figures
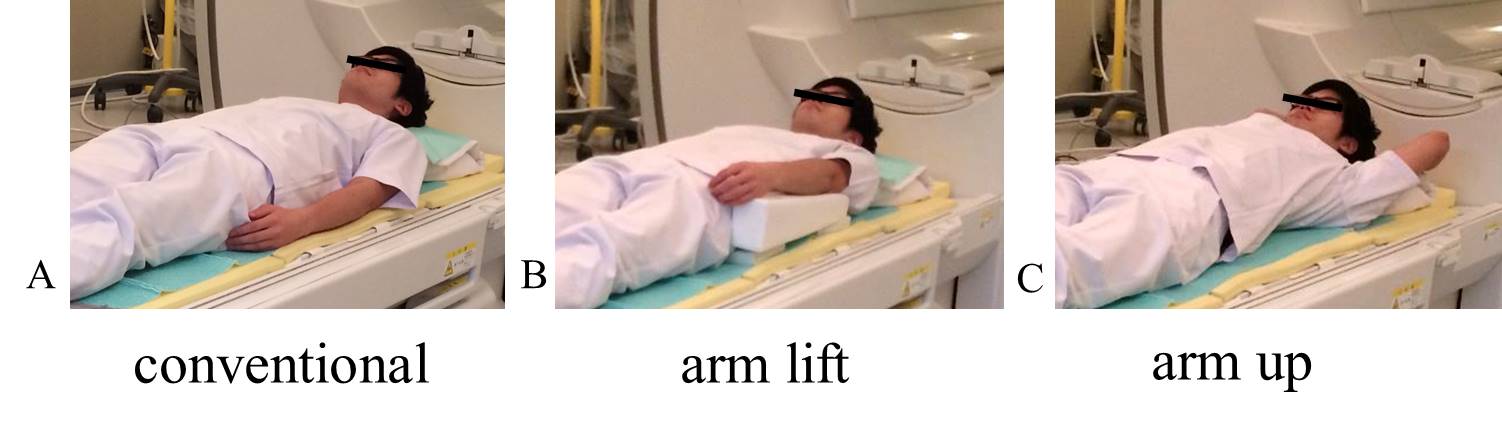
Fig.1 Arm positions.
Three kinds of arms positions are used in this study. A: conventional position (arms are on the bed), B: arm lift position (elevation of arms by 100 mm), C: arm up position (elevation of arm above the shoulder).
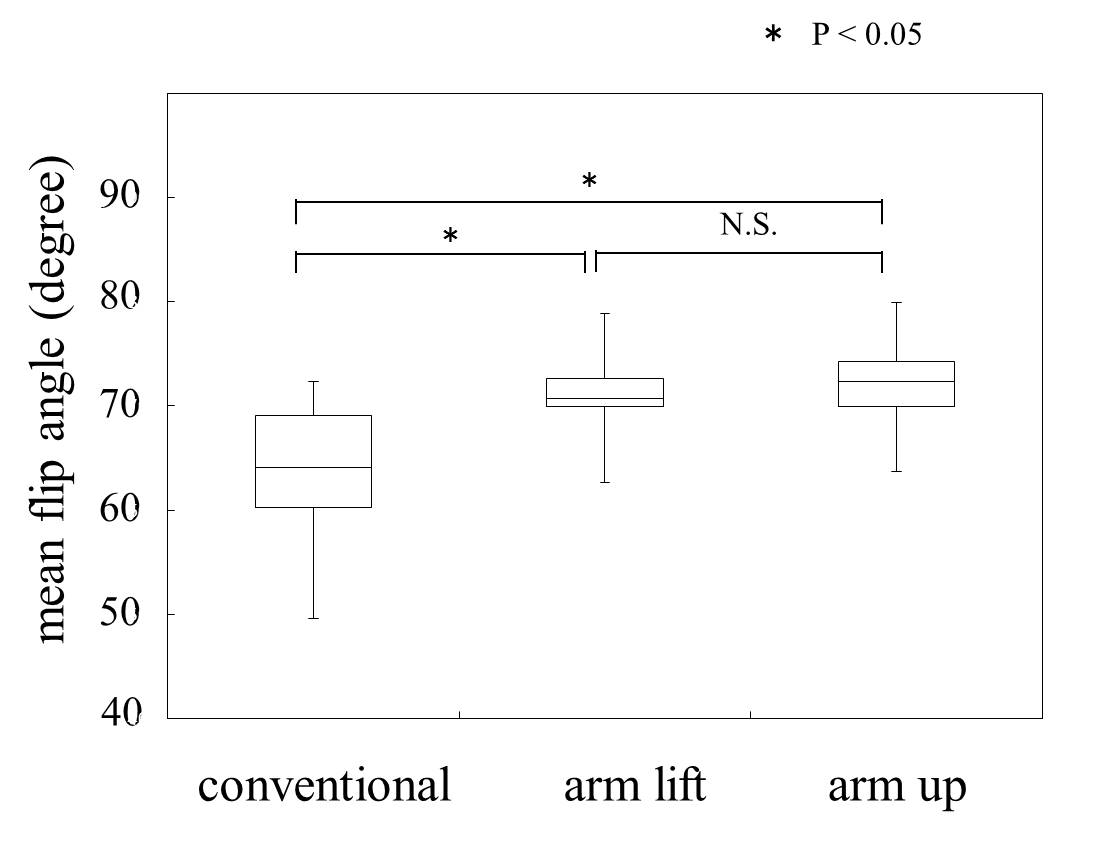
Fig.2 The mean of flip angles at Th12 level.
The mean flip angles of arm lift and arm up position are significantly higher than that of conventional position at Th12 level. The mean flip angles of arm lift position is not significantly different to that of arm up position.
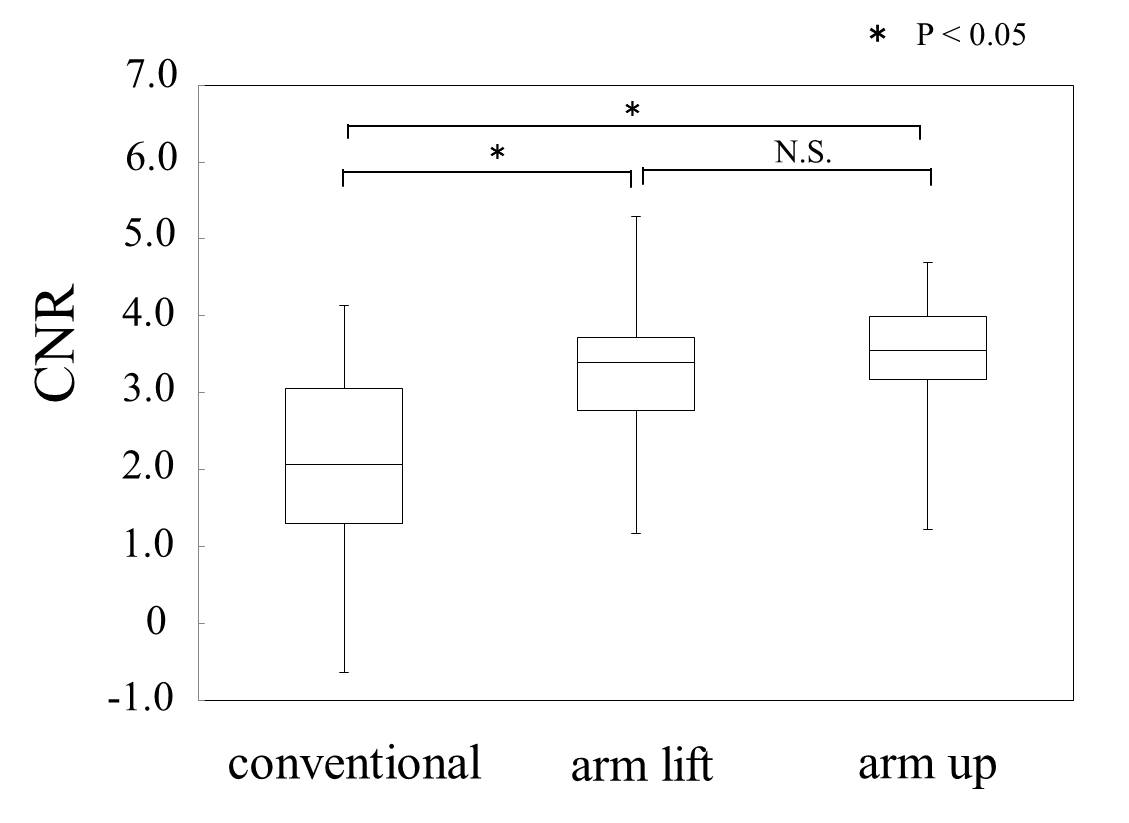
Fig.3 CNRs of spinal cord and CSF.
The contrast to noise ratio (CNR) of arm lift and arm up position are significantly higher than that of conventional position. The CNR of arm lift position is not significantly different to that of arm up position.
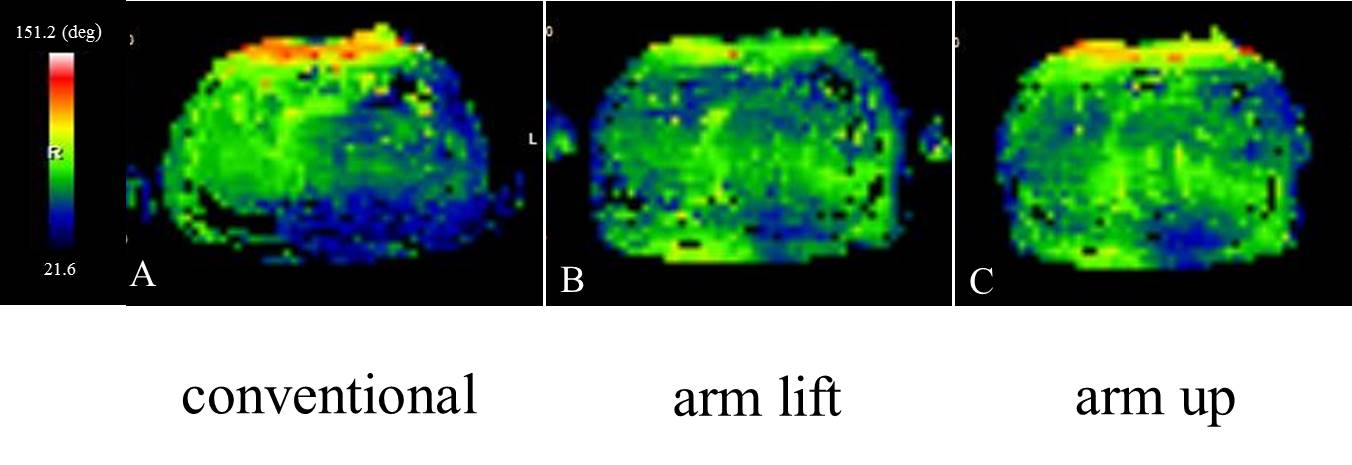
Fig.4 Examples of B1+ map at Th12 level.
In the B1+ map of the conventional position, vertebral regions are shown with almost blue color, indicating the under excitation of RF. However, those blue areas of vertebra are decreased in with the arm lift and arm up positions.
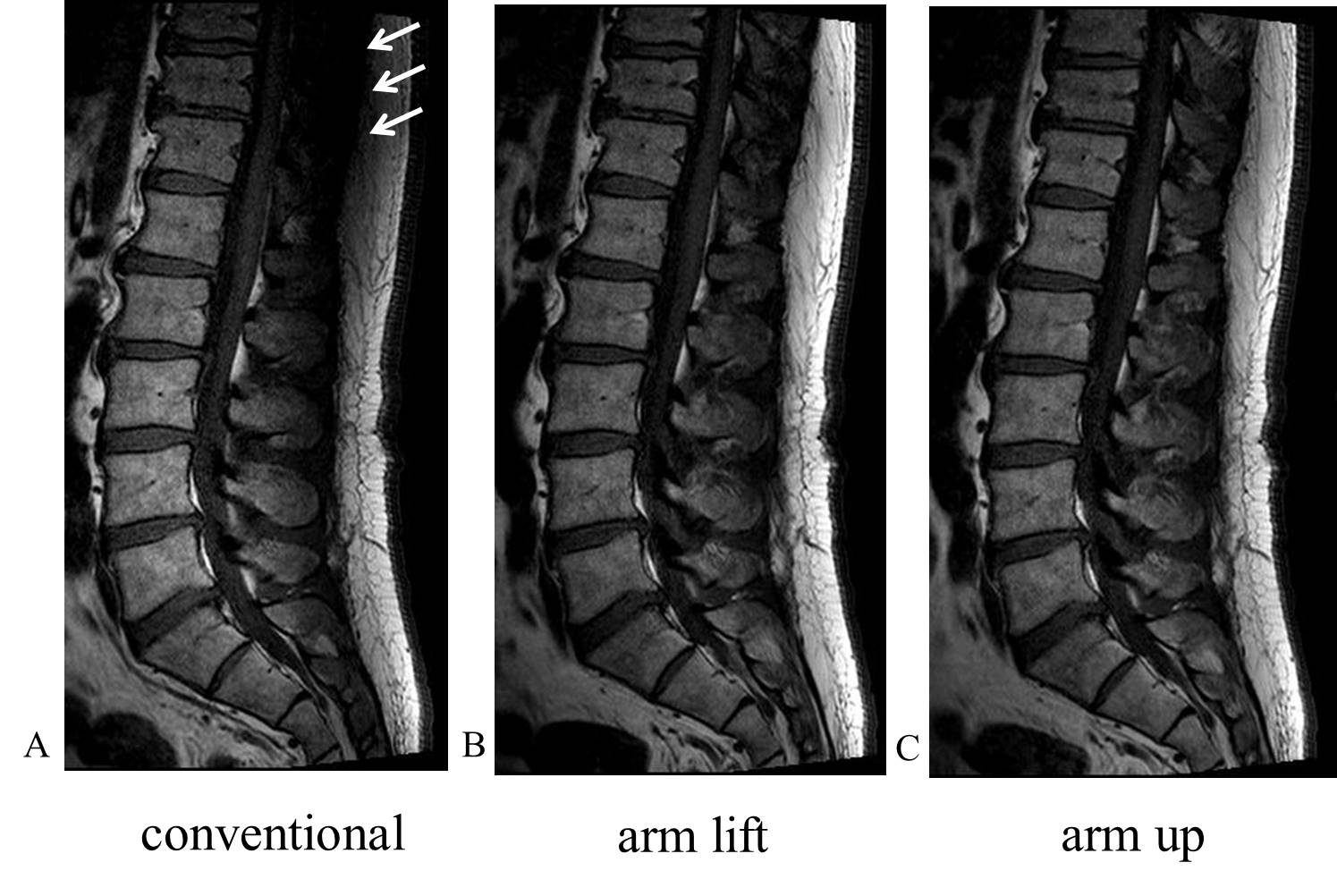
Fig.5 Examples of sagittal T1WI.
The signal intensities of the vertebral body, spinal cord, and spinous process at the range from Th11 to L1 of the conventional position are lower (white arrows), compared to the arm positions of arm lift or arm up.