4658
Does MR of the neck improve the credibility of victims after manual strangulation?1Ludwig Boltzmann Institute Clinical Forensic Imaging, Graz, Austria, 2Institute of Forensic Medicine, Medical University of Graz, Graz, Austria, 3Institute of Forensic Medicine, University of Basel - Health Department Basel, Switzerland
Synopsis
Former
studies have already shown, that MRI findings in victims after survived
strangulation allow the diagnosis of strangulation. Native 3T MR scans of the
neck were performed in strangulation victims without external findings. All
subjects showed strangulation specific MRI findings. Therefore, MRI of the neck
is indicated in cases of reported manual strangulation.
Introduction
The examination of survivors of manual or ligature strangulation is a common task in clinical forensic medicine. Actual gold standard in these cases is an external examination of the victim. Only in cases of clinical indication (i.e. difficulties in swallowing, hoarseness,) radiological evaluation is performed using CT. However, since survivors of strangulation often present only discreet or even absent external findings, the forensic assessment concerning the question if there really was a violent attack against the neck can be challenging. Former studies have shown that it is possible to detect findings mainly in the soft tissues, e.g. the subcutaneous tissue, muscles, and lymph nodes in the neck region after survived strangulation1,2. The aim of this study was to elucidate, if internal soft tissue injuries of the neck can be detected in victims of survived strangulation presenting without any external findings.Marterials & Methods
Native MRI scans of the neck (3T Trio, Siemens AG, Erlangen, Germany) of 12 subjects (Group A: 7 females, 4 male with a median age of 26.0, range 18.1-40.5 years) with a credible history of manual strangulation, but without any external injury of the head and neck (Fig.1) were performed (time between incident and MR Scan: 0-8 d). Additionally, MR scans of a control group consisting of 10 healthy volunteers (Group B: 5 females, 5 male) were done. All scans were conducted using a 12-channel head coil and a 4-channel neck coil (Matrix System, Siemens AG, Erlangen, Germany) with the following protocol [(T2w TSE, FS, TE/TR 87/7660ms, slice thickness 3.5-4mm, in 3 orientations) (T1w TSE, TE/TR 10/824ms, slice 3.5mm, coronal) (T1w TSE, FS, TE/TR 11-12/930-1020ms, slice 3.5mm, axial) (T1w MP-Rage, TE/TR 2.2/1800ms, slice 1mm, sagittal) (PDw FS, TE/TR=35/3540ms, slice 3mm, axial)]. The study was approved by the local ethics committee, written informed content was obtained from all study subjects. MR data were read by a board certified radiologist, experienced in forensic radiology, and blinded concerning the group membership of the subjects. Radiological findings were evaluated according a predefined diagnostic scheme3 including 5 criteria: vascular findings, bleeding into salivary gland, bleeding into lymph node, bleeding into muscle and subcutaneous edema or bleeding. For the diagnosis of strangulation at least one of these criteria had to be present.Results
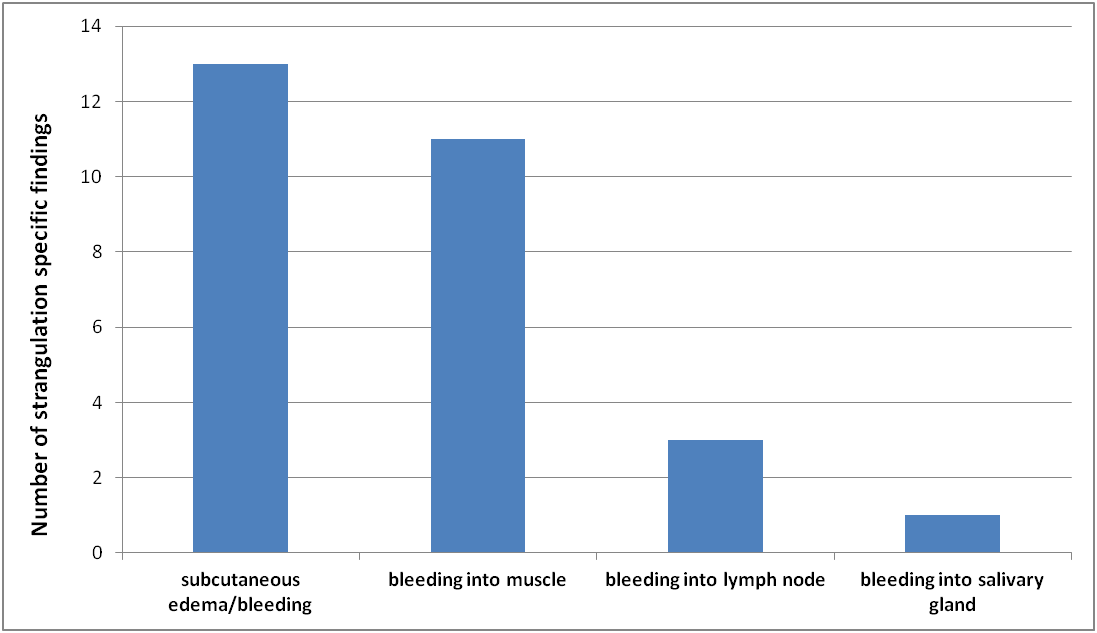
All 12 subjects of Group A showed MR findings. In total the radiological evaluation detected 51 findings of which 28 were considered as specific for strangulation as they met the criteria of the above-mentioned diagnostic scheme. The other 23 findings did not meet these criteria (e.g. hypertrophy of lymph nodes, thyroid nodules, degeneration of intervertebral disks). The majority of the findings could be assigned to the criterion subcutaneous edema or bleeding (n=13) . Furthermore, a considerable number (n=11) of bleedings into muscle tissue, mainly the sternocleidomastoid muscle, was detected.(Fig.2) Bleedings into lymph nodes were found in three cases, and one subject showed a bleeding into a salivary gland (Fig.3) . In all controls (Group B) no findings according to the above mentioned criteria were detected in the radiological evaluation.Discussion & Conclusion
Survivors of strangulation often show no external findings and therefore their report of violence against the neck cannot be based on objective findings. Strangulation specific signs, determined in a predefined scheme, were detected in non-enhanced 3T MRI in all victims, who showed no strangulation typical external findings. These strangulation specific inner findings are soft tissue findings which cannot be seen in CT, as it is performed in clinical routine in case of medical indication - a fact that ascribes enormous importance to MRI regarding to diagnose strangulation based on objective findings. Based on the results of this study it is recommended to perform a native MR scan of the neck in cases of reported manual strangulation in order to improve the credibility especially in victims without external findings.Acknowledgements
No acknowledgement found.References
1. Yen et al. Clinical forensic radiology in strangulation victims: forensic expertise based on magnetic resonance imaging (MRI) findings. Int J Leg Med 2007;121:115-123.
2. Christe et al. Life-threatening versus non-life-threatening manual strangulation: are there appropriate criteria for MR imaging of the neck? Eur Radiol 2009;19:1882-9.
3. Pivec et al. Identification of living victims of manual strangulation by MR imaging of the neck. Proc ISMRM 2012.
Figures
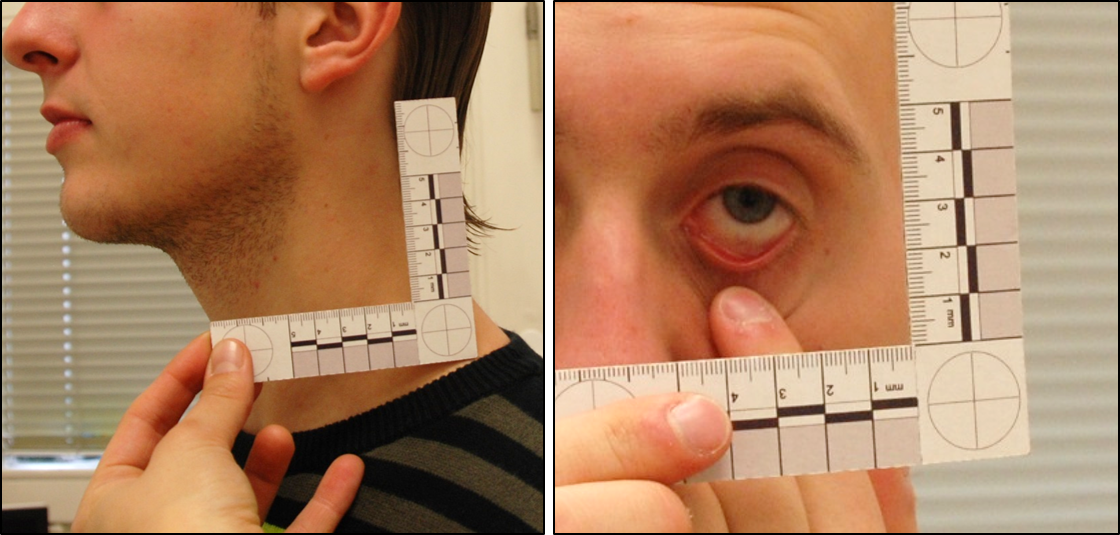
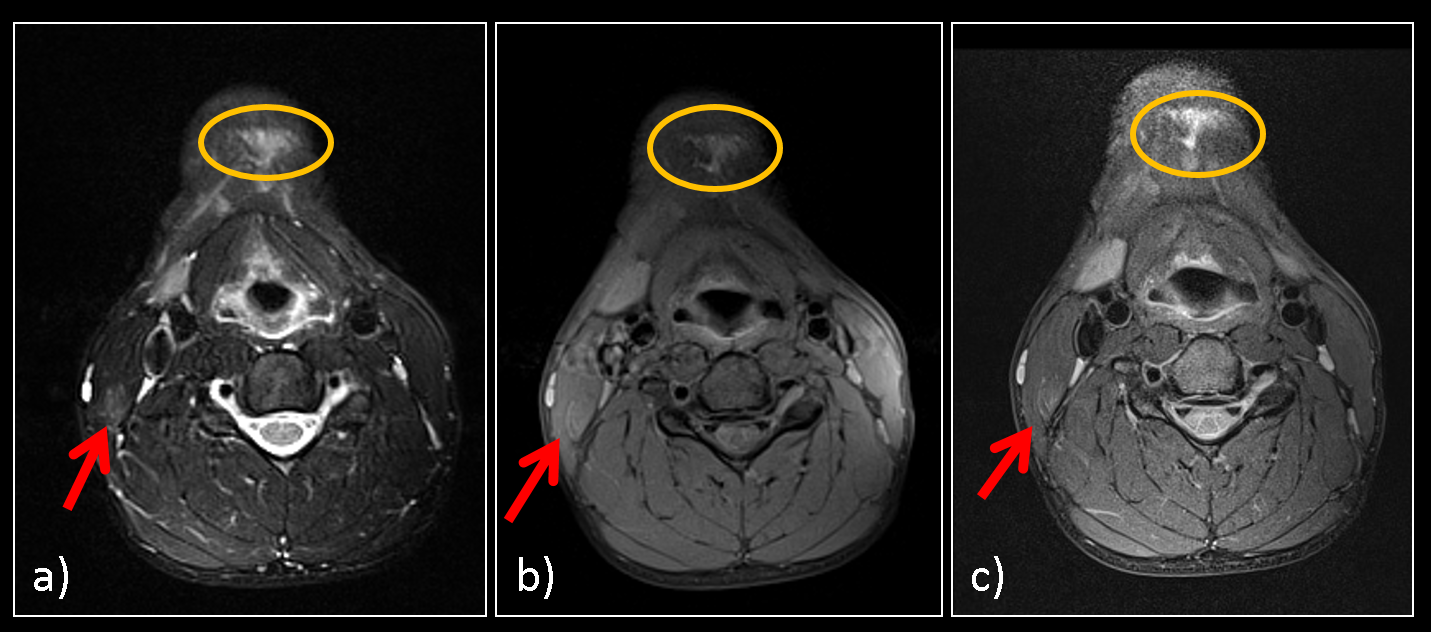
Fig.2: MRI findings of the victim presented Fig. 1: submental subcutaneous edema (circle) and bleeding in the right sternocleidomastoid muscle (arrow); a) T2w TSE FS, b) T1w TSE FS, c) PDw TSE SPAIR