4617
Stable CBF fluctuation in 4-day follow up after carotid artery stenting compared with carotid endarterectomy revealed by 3D pCASL1Radiology, Chinese PLA General Hospital, Beijing, People's Republic of China, 2GE healthcare China
Synopsis
Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are two commonly used surgical treatment methods for severe internal carotid artery (ICA) stenosis, hence, our objective was to investigate the CBF difference before and in 4-day follow up after CEA and CAS using 3D pCASL technique. As it demonstrated, the CBF values showed no significant (P>0.05) differences in various time points prior to the operations between CAS and CEA, whereas compared to the patients after CEA, the CBF values were stable fluctuated in various time points (P<0.05). This proves that 3D pCASL is useful for quantifying CBF changes after CAS or CEA; moreover, the stable fluctuation CBF may indicate that CAS has a lower hyperperfusion syndrome and death rate compared to CEA in the future.
Purpose
In patients with a severe symptomatic internal carotid artery (ICA) stenosis, carotid endarterectomy (CEA) as well as carotid artery stenting (CAS) are two commonly used surgical treatment methods1. It has been reported that CEA may feature a lower rate of death and stroke as compared to CAS2, but others thought there was no difference in cerebral hemodynamic effect between both approaches3. Hence, the aim of this study is to investigate the cerebral blood flow (CBF) differences in patients before and in 4-day follow up after CEA and CAS as revealed by 3D pseudocontinuous arterial spin labeling (pCASL) .Methods and Materials
Thirty-four patients were diagnosed with moderate to severe ipsilateral internal carotid artery stenosis by referring clinicians were enrolled in this study. Twenty patients underwent CAS (male, 16; age, 64.4±11 years) and fourteen underwent CEA (male, 11; age, 61.8±9.8 years). All the subjects underwent MRI scans consisting of MRA, DWI and ASL on 3.0T whole body scanner. Five scans were performed including pre-operation, the first day, the second day, the third day and the forth day after operation. CBF measurements were made in regions of ipsilateral ICA territory based on ASL raw data images, including gyrus of frontal and parietal lobe, centrum semiovale, gyrus of temporal lobe, head of caudate nucleus, and the region of posterior circulation territory, such as cerebellar hemisphere (Figure 1). Unpaired t-test was performed to compare the significance of the inter-group difference in CBF values.Results
The histogram of CBF values of CEA and CAS at different time points is shown in Figure 2. No statistically significant (P>0.05) difference of CBF was observed in various regions of patients who received CEA or CAS, prior to the operations. However compared to the patients who received CEA, CBF values were observed to be stable fluctuated in various time points as compared to patients who received CAS: on the first day in the gyrus of frontal and parietal lobe (P=0.000), centrum semiovale(P=0.005), gyrus of temporal lobe(P=0.000), head of caudate nucleus(P=0.000) and cerebellar hemisphere(P=0.000); the second day in the gyrus of frontal and parietal lobe(P=0.001), centrum semiovale(P=0.001), gyrus of temporal lobe(P=0.000), head of caudate nucleus(P=0.004) and cerebellar hemisphere(P=0.000); the third day in the gyrus of frontal and parietal lobe(P=0.003), centrum semiovale(P=0.007), gyrus of temporal lobe(P=0.006), head of caudate nucleus(P=0.049) and cerebellar hemisphere(P=0.001) and the forth day in the gyrus of frontal and parietal lobe(P=0.000), centrum semiovale(P=0.006), gyrus of temporal lobe(P=0.001), head of caudate nucleus(P=0.004) and cerebellar hemisphere(P=0.001) (Table 1, Figure 2).Discussion and Conclusion
The choice between CAS or CEA has been an ongoing debate, however no evidence has been provided up to date on the competiveness between the two. In this work, the CBF assessed using ASL was used as a metric for comparison in patients who underwent the two procedures. Comparatively stable fluctuation CBF was observed in patients who underwent CAS, which indicates that CAS has a lower hyperperfusion syndrome and death rate compared to CEA in the future.Acknowledgements
We would like to acknowledge Zhenyu Zhou, PhD, Bing Wu, PhD, at GE Healthcare, Beijing, China, for their excellent technical assistance.References
1. Dimitrios Christopoulos, Eugenios Philippov. The results of a simplified technique for safe carotid stenting in the elderly. J Vasc Surg 2011;54:1637-1642.
2. Ringleb PA, Allenberg J, Bruckmann H, et al. 30 day results from the SPACE trial of stent- protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial. Lancet 2006;368:1239-1247.
3. Peter Jan Van Laar, Jeroen Hendrikse, Willem P. Th. M. Mali, et al. Altered flow territories after carotid stenting and carotid endarterectomy. J Vasc Surg 2007;45:1155-1161
Figures
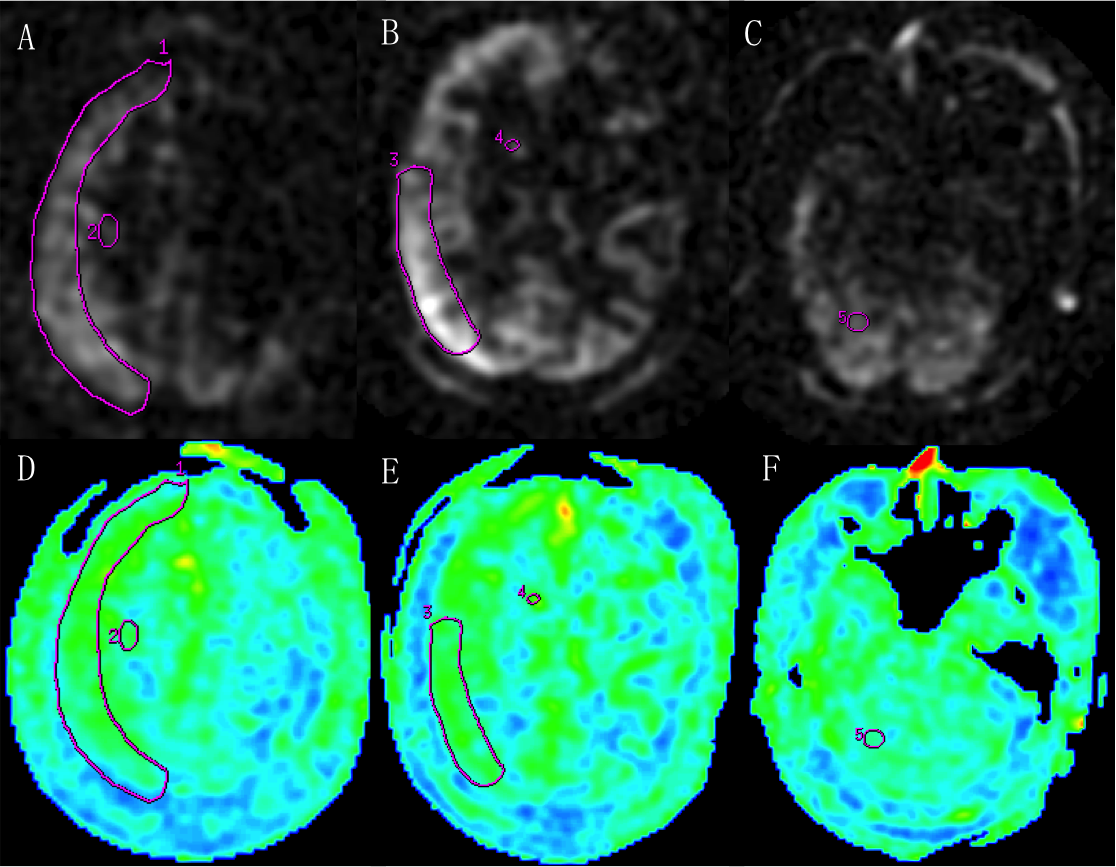
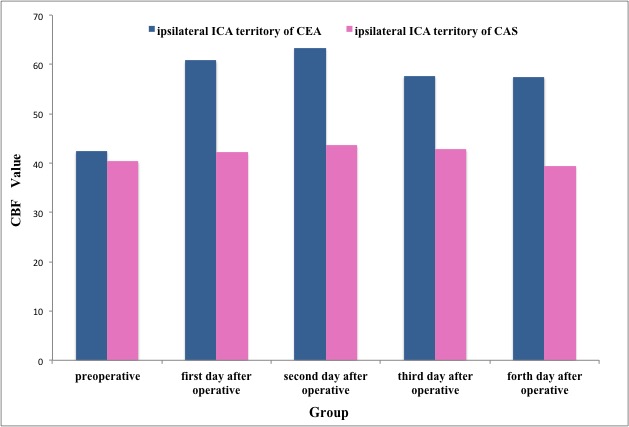
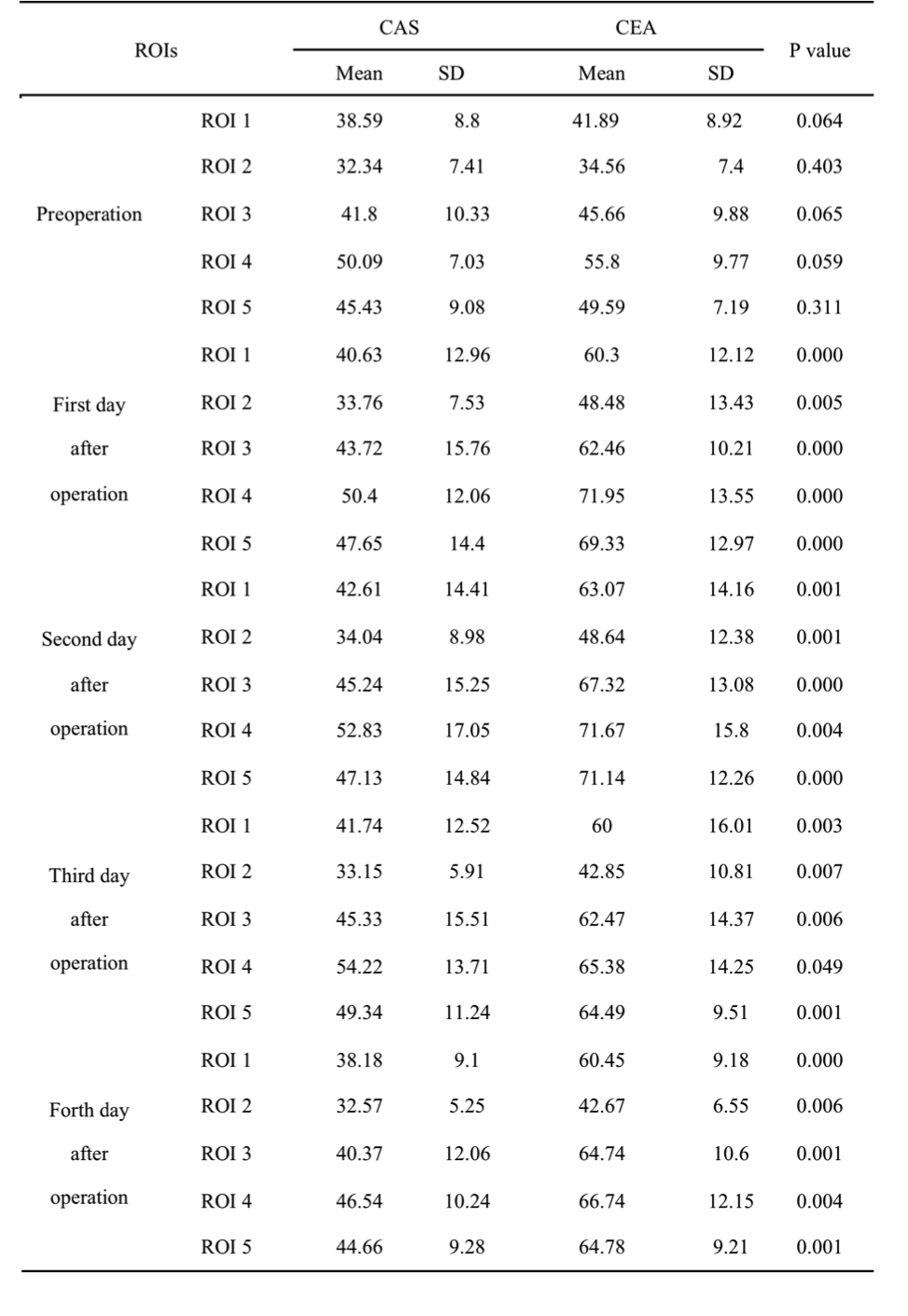
Table 1. Mean CBF values and standard deviation (SD) between various time points in patients underwent CEA and CAS.
ROI 1: gyrus of frontal and parietal lobe, ROI 2: centrum semiovale, ROI 3: gyrus of temproal lobe, ROI 4: head of caudate nucleus, ROI 5: cerebellar hemisphere