4605
Changes in fMRI activation pattern during different levels of sacral nerve stimulation for overactive bladder1Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 2Glickman Urology & Kidney Institute, Cleveland Clinic, Cleveland, OH, United States, 3Urogynecology Unit, H. Dr. Sotero del Rio, Santiago, Chile, 4Division Obstetricia y Ginecologia, Pontificia Universidad Católica de Chile
Synopsis
Sacral nerve stimulation (SNS) is an effective treatment for refractory overactive bladder(OAB). For patient-specific and therapeutic efficacy, stimulus at levels below or above the sensory level are sometimes applied on OAB patients. Previous functional brain studies suggested that few forebrain circuits acting primarily on midbrain periacqueductal grey is responsible for facilitating voiding reflex and a sensation of voiding. The neural circuits underlying the action of SNS, and its response to different levels of stimulus is studied by functional MRI (fMRI). Differences in activation patterns resulting from subsensoy, sensory and supresensory stimulation are reported.
Purpose
Sacral
nerve stimulation(SNS) is an effective treatment for refractory overactive
bladder(OAB)1. Its mechanism of
action is unknown, but likely involves spinal reflexes and afferent signaling
to the brain. Based upon functional brain imaging studies, few forebrain
cricuits, acting primarily on midbrain periacqueductal grey (PAG), have been
proposed to facilitate the voiding reflex and generate a sensation of voiding2. The effects of
SNS at, above, and below stimulus sensory threshold level on fMRI-measured
brain activity in OAB were measured in this study to identify the neural circuits
involved in SNS therapy.
Methods
Following Institutional Review Board (IRB) approval, women with non-neurogenic refractory OAB who (i) responded well to SNS via Medtronic InterStim II device, (ii) had a stable program for 3 or more months, and (iii) received no adjuvant OAB treatment were recruited. Enrolled patients completed pre-fMRI validated symptom and quality of life instruments [Urogenital Distress Inventory (UDI)-6, Incontinence Impact Questionnaire (IIQ)-7, Patient Global Impression of Severity (PGI-S), and Perceived Urgency Intensity (PUI)]. Stimulus settings were recorded, devices were switched off for a 5-day washout, and the instruments were repeated. A total of 3 fMRI scans below (sub-sensory), at (sensory), and above (supra-sensory) stimulus sensory threshold level were done. Sub-sensory voltage was set at the amplitude below which the subject could not feel the stimulation, while the supra-sensory voltage was set at the amplitude above which the subject would feel uncomfortable. The stimulators were set at 1.8±0.7 V [range: 1.1-3.0 V] (sub-sensory), 2.4±1.0 V [range: 1.5-3.7 V] (sensory) and 3.7±1.1 V [range: 2.5-4.8 V] (supra-sensory), while the frequency and pulse-width were maintained at 14 Hz and 210 µs for all subjects.
Patients were scanned in a 3 tesla whole body Prisma scanner (Siemens, Erlangen, Germany). The fMRI scan consisted of a 2D gradient echo echo-planar sequence (TR/TE=2800/29 ms, FOV=256×256 mm2, matrix size=128×128, slice thickness=4 mm) and was acquired over 5 stimulator OFF and 4 stimulator ON cycles of 42 seconds each. The subjects were trained outside the scanner to respond to each change of state between ON/OFF and report this with a response button during the fMRI scans. The patient responses closely matched with the ON/OFF state changes as expected from the stimulator programming. fMRI data were analyzed using AFNI software package3, and consisted of (i) rejecting 1st 4 points of the time-series, (ii) physiologic noise correction using 3D RETROICOR4, (iii) retrospective motion correction using 3dvolreg, (iv) spatial filtering using a 64-point radially symmetric Hamming in the Fourier domain, and (ii) Student t activation map generation using 3dDeconvolve. Output images use single voxel p-value 0.05 with false positive error of 0.05 (cluster-analysis determined). Average maps under the 3 settings of the stimulus viz. (i) sub-sensory, (ii) baseline, and (iii) supra-sensory were produced.Results and Discussion
Out
of 13 enrolled patients 3 did not undergo MRI and 3 were excluded for poor OAB
symptom control. The remaining 7 subjects were scanned for fMRI. Data from one
subject had to be excluded for possible hardware related issues, and the
remaining 6 subjects’ data were analyzed. The sample had a median age 52[36-64]
years. Urinary bother significantly worsened with ‘washout’ while symptoms
worsened with a trend toward significance. Voiding diary data supported these
findings. After fMRI all devices had normal impedances and there were no
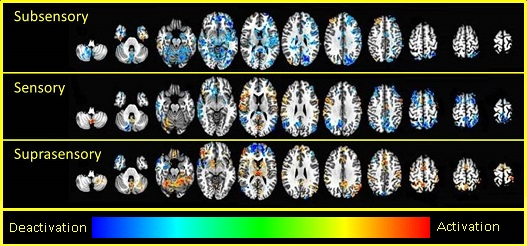
changes in PUI (p0.363) or PGI-S (p0.363) from baseline. An overall pattern of
brain activation generally progressed with increasing stimulation, but
activation of the right inferior frontal gyrus remained stable, while
deactivation of the pons and PAG matter was only noted with sub-sensory
stimulation (Fig. 1). Sensory stimulation activated the insula but deactivated
the medial and superior parietal lobes. Suprasensory stimulation activated
multiple structures and the expected S3 sensory region. While SNS stimulation
related S3 nerve stimulation resulting in activation of cingulate gyrus, PAG,
amygdala and insula has previously been reported5, 6, this constitutes the first effort to study fMRI
activation pattern with different stimulator settings. This enables not only to
explore the pathway of SNS action, but also to investigate how changes in
stimulator settings might change the brain activation; this is important to
study since some patients respond to stimulation at a sub-sensory level due to
inability to tolerate the stimulus sensation, while some patients need
increased amplitude (supra-sensory) to derive a therapeutic effect.
Conclusion
Varying SNS influences fMRI activation pattern. These results suggest SNS may have a centrally-mediated mechanism of action.Acknowledgements
Funded via unrestricted Medtronic Research Grant.References
Figures