4589
Altered structure and functional connectivity of the post-insular in uremic restless legs syndrome patients1Radiology Department, First Affiliated Hospital of Xi’an Jiaotong University, XI'AN, People's Republic of China
Synopsis
To investigate the structure and functional changes in the insulars in uremic RLS patients using a resting-state function magnetic resonance imaging (fMRI )paradigm,We examined cortical thickness,and investigage the abnormal functional connectivity in maintenance dialysis patients. The clinical parameters and RLS severity were correlated analyzed. The characteristics of uremic RLS patients were compared to those of the controls.
Synopsis
To investigate the structure and functional changes in the insulars in uremic RLS patients using a resting-state function magnetic resonance imaging (fMRI )paradigm,We examined cortical thickness,and investigage the abnormal functional connectivity in maintenance dialysis patients. The clinical parameters and RLS severity were correlated analyzed. The characteristics of uremic RLS patients were compared to those of the controls.
Method
29 ESRD patients on hemodialysis with restless legs syndrome and 27 age- and gendermatched control individuals (without renal or neurological problems) underwent T1-weighted, resting state fMRI and clinical assessments. Freesurfer was used to perform vertex-wise comparisons of cortical thickness, whereas the seed-based method was implemented to construct and analyze the functional connectivity.The clinical parameters and RLS severity were correlated analyzed. The characteristics of uremic RLS patients were compared to those of the controls.Result
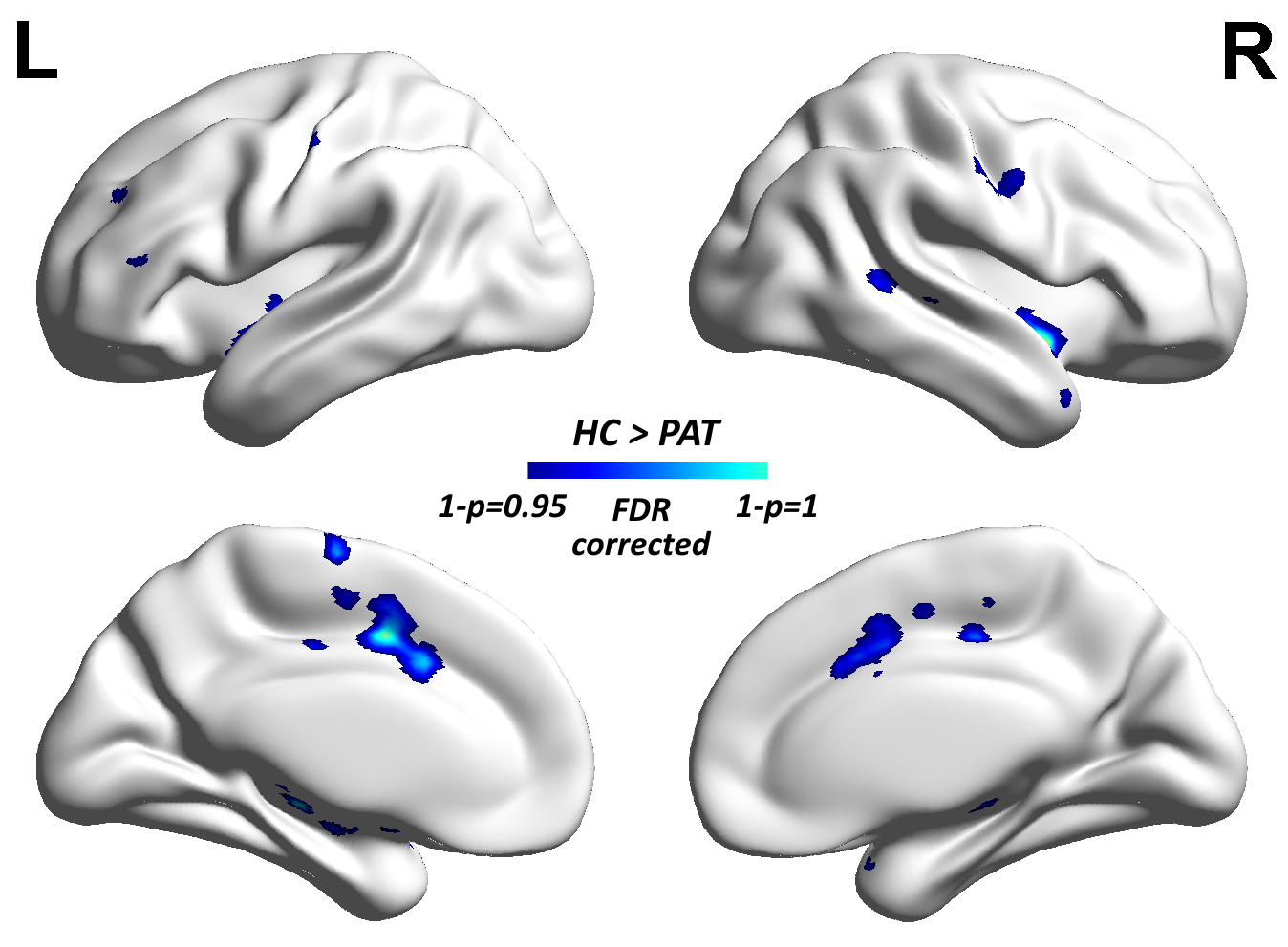
Our results suggest that the decreased left posterior insular cortical thickness and \that reduced right connectivity with the right hippocampus gyrus, bilateral precentral
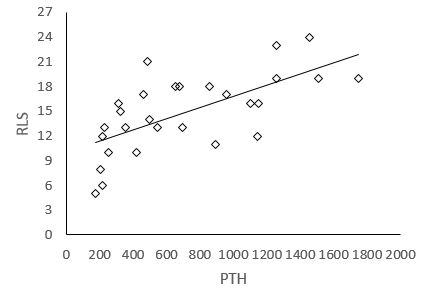
gyrus, bilateral posterior insulars, bilateral sensorimotor cortex and middle cingulate cortices. may reflect the pathways involved in producing uremic RLS symptoms. RLS severity was positively correlated with hemodialysis duration (P<0.05) and negatively correlated with parathyroid hormone(PTH).
Discussion
Even though there are several studies reporting the functional connectivity of the insular with the cingulated cortex, its relationships with other brain areas remain elusive in uremic RLS. Therefore, we decided to use rsFC to elucidate in details its connectivity, in terms of cortical and subcortical areas, and also of lateralization. in this study,we observed decreased thickness in the left posterior insrlar among uremic RLS patents.Generally,the posterior insula connects reciprocally with the secondary somatosensory cortex and receives input from spinothalamically activated ventral posterior inferior thalamic nuclei. It has also been shown that this region receives inputs from the ventromedial nucleus (posterior part) of the thalamus that are highly specialized to convey homeostatic information such as pain, temperature, itch, local oxygen status, and sensual touch.But we could not find the abnormal conectivity between posterior insula and thalamus,which suggested that the emergence of RLS symptom may be in consequence of the sensorimotor network(SMN) associated left posterior insula.
the ventralanterior insula in humans is functionally connected to the anteriorcingulate (ACC) and frontal cortices, whereas the dorsal posteriorinsula is linked to motor, somatosensory, and temporal cortices. The potential pathophysiology of this disease consists of hemodialysis, dopaminergic system dysfunction, brain iron deficiency, and calcium/phosphate imbalance, which may appear in end-stage kidney disease patients easily. We found the connectivity reductions were located in sensorimotor areas, and the RLS severity was positively correlated with hemodialysis duration, both of them indicated the lower function of sensorimotor of uremic patients. Compared with normal group, the decreaed connectivity including the right hippocampus gyrus, bilateral precentral gyrus, bilateral posterior insulars, bilateral sensorimotor cortex and middle cingulate cortices, which are the parts of sensorimotor network (SMN) . These findings support the SMN, a system underlying motorcontrolling and movement executing, may affected in uremic RLS. Function connectivity (FC)can measures the temporal correlations of spontaneous fluctuations in brain activity between spatially remote regions, the seed based resting-state functional magnetic resonance imaging (rs-fMRI)paradigm could provide much more precise and detailed look at specific connectivity of insula with other region of brain.
The decreased connectivity was with the correlation of PTH, While PTH acts to increase the concentration of ionic calcium(Ca2+) in the blood, calcitonin, a hormone produced by the parafollicular cells (C cells) of the thyroid gland, acts to decrease ionic calcium concentration.calcium/phosphate imbalance is alsoreported to be involved in the pathophysiology of uremicRLS.
Conclusions
In
conclusion, the present study applied morphometry analysis and resting-state
functional connectivity to examine the structural and functional integrity
changes of insula in uremic RLS patients. Our findings document that patients with RLS
undergoing hemodialysis display clear-cut structural alterations in left posterior insula. Moreover, altered resting state functional connectivity with sensorimotor network. Increased PTH may be a key factor of uremic RLS patients undergoing hemodialysis.Acknowledgements
We wish to thank all the subjects who participated in this study.This research work is supported by the National Natural Science Foundation of China(NO.81571640)References
1. Giannaki CD, Hadjigeorgiou GM, Karatzaferi C, Pantzaris MC, Stefanidis I, Sakkas GK. Epidemiology, impact, and treatment options of restless legs syndrome in end-stage renal disease patients: an evidence-based review. Kidney international 2014;85:1275-1282.
2. Kavanagh D, Siddiqui S, Geddes CC. Restless legs syndrome in patients on dialysis. American journal of kidney diseases : the official journal of the National Kidney Foundation 2004;43:763-771. 3. Kawauchi A, Inoue Y, Hashimoto T, et al. Restless legs syndrome in hemodialysis patients: health-related quality of life and laboratory data analysis. Clinical nephrology 2006;66:440-446.
4. Seifter J, Samuels M. Uremic Encephalopathy and Other Brain Disorders Associated with Renal Failure. Seminars in Neurology 2011;31:139-143.
5. Winkelman JW, Gagnon A, Clair AG. Sensory symptoms in restless legs syndrome: the enigma of pain. Sleep Med 2013;14:934-942.
6. Rijsman RM, de Weerd AW, Stam CJ, Kerkhof GA, Rosman JB. Periodic limb movement disorder and restless legs syndrome in dialysis patients. Nephrology 2004;9:353-361.
7. Rizzo G, Tonon C, Manners D, Testa C, Lodi R. Imaging brain functional and metabolic changes in restless legs syndrome. Current neurology and neuroscience reports 2013;13:372.
Figures