4576
Study on the correlation between carotid bifurcation anatomy and atherosclerotic plaque by high resolution MR1Tianjin 4th Center Hospital, Tianjin, People's Republic of China, 2Philips Healthcare, Beijing, People's Republic of China
Synopsis
Based on carotid MR imagings performed on a 3.0T MR scanner with an eight-channel phased-array carotid coil, including 3D TOF, BB-T1WI, BB-T2WI, 3D MP-RAGE, 3D MERGE, We investigated the characteristics of the internal carotid artery angle and common carotid artery bifurcation angle, and compare different forms of carotid bifurcation, analyzed the occurrence of the vulnerable plaques and plaque components, found that bifurcation angles of the internal carotid artery and the common carotid artery have a close relationship with the occurrence of atherosclerosis. Vulnerable plaque with LRNC is more likely to occur at the large angle of the internal carotid artery.
Objective
To investigate the characteristics of the internal carotid artery angle and common carotid artery bifurcation angle, and compare different forms of carotid bifurcation, furtherly to investigate the relationship between the anatomy of carotid artery bifurcation and the composition of carotid atherosclerotic plaque.Methods
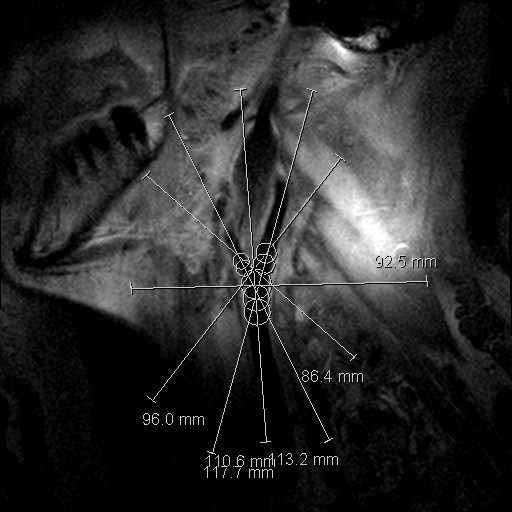
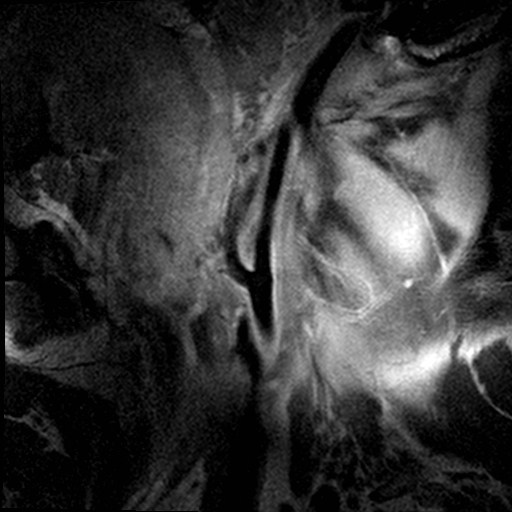
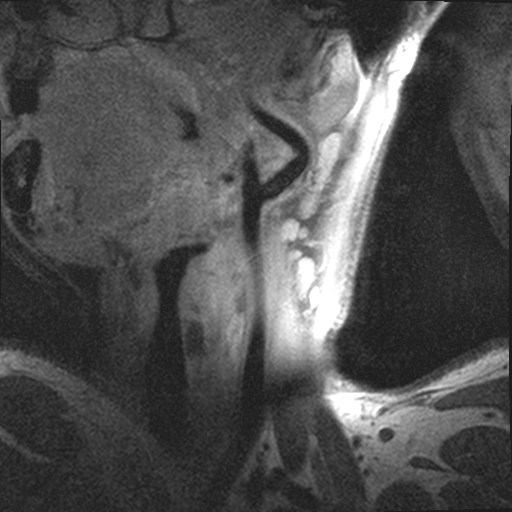
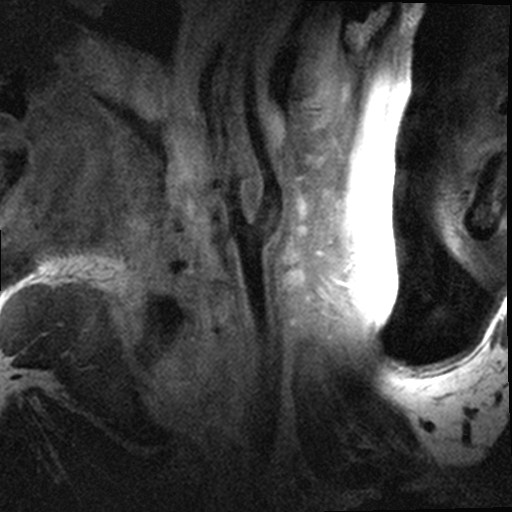
One hundred and fourteen-four patients (male 68, female 46, age 41-85 years old) with carotid artery stenosis were recruited in this study. The carotid MR imaging was performed on a 3.0T MR scanner (Achieva TX, Philips Healthcare, Best, the Netherlands) with an eight-channel phased-array carotid coil, centering on the bifurcation of the symptomatic carotid arteries, which are defined as the arteries responsible for the neurological symptoms. We acquired the cross-sectional carotid MR images with the following parameters: (1) 3D time of flight (TOF), TR/TE=20/5.1 ms, flip angle= 20 degree; (2) quadruple inversion-recovery T1W sequence based on TSE, TR/TE= 800/10 ms; (3) T2W sequence with multi-slice double inversion recovery, TR/TE=4000/50 ms; (4) 3D MP-RAGE sequence based on IR-TFE, TR/TE =9.2/5.5 ms, flip angle= 15 degree;(5)3D MERGE sequence based on IR-TFE, TR/TE =9.2/5.5 ms, flip angle= 6 degree. All carotid MR axial images were acquired with a FOV = 14× 14 cm, slice thickness = 2 mm, acquisition matrix = 256 × 256, and longitudinal coverage =32 mm (16 slices). All recruited subjects were divided by two ways[1,2]: 1) According to size of internal carotid artery angle and the common carotid artery bifurcation angle, recruited subjects were divided into Large Angle Group (LAG) and Small Angle Group (SAG). 2) According to the carotid bifurcation form, recruited subjects were divided into straight bifurcate, straight bent and bent bifurcate groups(Figure 1-4). We analyzed the occurrence of the vulnerable plaques and plaque components for each group, and compared the difference among these groups through chi-square test method by using IBM SPSS Statistics 17.0 (Armonk, New York, USA) and P<0.05 indicated a significant difference.Results
Significant difference was found in incidence of vulnerable plaques between LAG and SAG (50.5% vs 36.6 %, p<0.05), and only lipid-rich necrotic core (LRNC) occurrence were found significant difference between the two groups (χ2=3.947, p<0.05). No clear statistic difference was found among three carotid artery bifurcation forms.Discussion
Compared with the common carotid bifurcation angle, the contribution of internal carotid artery angle to plaque is even greater. The reason may be that the common carotid artery bifurcation angle includes parts of external carotid artery angle which would affect the blood flow evaluation. But the internal carotid artery angle can accurately reflect the blood flow state[3]. There was no statistical difference in the correlation between three carotid artery forms and plaque, which may be due to the influence of individual factors on evaluation of carotid artery morphology, which needs further investigation.Conclusion
The bifurcation angles of the internal carotid artery and the common carotid artery have a close relationship with the occurrence of atherosclerosis. Vulnerable plaque with lipid-rich necrotic core is more likely to occur at the large angle of the internal carotid artery. The carotid bifurcation form has no direct relationship with the occurrence of atherosclerosis plague.Acknowledgements
This research was supported by a research fund from Tianjin Public Health Bureau(14KG113).
References
1. Satoshi Daitoku, Toshinori Yuasa, Hiroshi Tsunenari, et al. Angle between the common and internal carotid arteries detected by ultrasound is related to intima-media thickness among those with atherosclerotic disease. Environ Health Prev Med (2015) 20:216–223.
2. Matthias Sitzer, Damir Puac, Alexandra Buehler, et al. Internal Carotid Artery Angle of Origin A Novel Risk Factor for Early Carotid Atherosclerosis. Stroke. 2003 Apr;34(4):950-5.
3. Michael Markl, Felix Wegent, Timo Zech, et al. In Vivo Wall Shear Stress Distribution in the Carotid Artery Effect of Bifurcation Geometry, Internal Carotid Artery Stenosis, and Recanalization Therapy. Circ Cardiovasc Imaging. 2010;3: 647- 655.
Figures