4457
Whole-body MRI for initial assessment of plasma cell disorders including multiple myeloma1University College London, London, United Kingdom, 2University College London Hospital, United Kingdom, 3University College London, 4University College London, United Kingdom
Synopsis
Whole body MRI (WB-MRI) is increasingly being used to assess plasma cell disorders (PCDs). The adoption of WB-MRI provides a niche to further incorporate novel imaging technique into assessment of PCDs, streamlining decision making progress in a cost-effective way.
Clinical Question:
To adopt whole-body MRI for initial assessment of plasma cell disorders (PCDs) including multiple myeloma (MM)Impact:
Currently, the initial assessment of PCDs consists of a wide range of biochemical and imaging investigations [1]. For imaging investigations, a combination of skeletal survey, CT scan, PET-CT and whole-spine MRI (WS-MRI) is usually adopted [1-3]. In the past decade, whole-body MRI (WB-MRI) is increasingly being used for baseline assessment of PCDs due to its superior diagnostic ability compared to multi-modality imaging [4-7]. There is still no accepted uniform imaging protocol for WB-MRI in PCDs despite the adoption of technique by various institutions and guidelines [8] for use in early detection [9] and potential prognostication [9,10]. The lack of an agreed protocol limits the generalizability and wider adoption of this technique. The potential advantage of WB-MRI is not limited to diagnosis. The limited resources and financial strains in modern medicine era necessitate the adoption of ‘cost-effective’ diagnostic procedures. Table 1 provides an estimate of the cost of current imaging techniques available for the assessment of MM in the UK. In addition, the adoption of WB-MRI for MM evaluation might reduce the use of additional imaging modalities (such as skeletal survey, PET etc), and this in turn may save money and speed up clinical decision-making. For instance, because WS-MRI is commonly required for assessment of the axial skeleton for fracture and neural compression, a combined single-session MRI approach (WB-MRI + WS-MRI) could well be preformed in a reasonable time using modern MRI scanners. Such approach has been previously tested for local and metastatic staging of prostate cancer [11].Approach:
Standard approaches for PCD assessment are based on ‘global measure’ of disease and its response following chemo/radiotherapy. The conventional imaging techniques (skeletal survey, CT) are not sensitive for detection of bone disease, especially at early stages of disease [12]. Despite its enhanced diagnostic ability; PET-CT imparts a substantial radiation exposure to patients [13,14]. Furthermore, PET-CT is not readily available in all institutions (health equality) and compared to WB-MRI, it is more expensive. Whole-spine MRI is now an integrated imaging technique for detection of disease and assessing the risk of insufficiency fracture [2,3,12], however, performed alone, it can miss up to 50% of bone lesions because of its limited coverage [12]. To increase patient comfort, decrease the cost, and increase effectiveness, we have designed, modified and updated a WB-MRI protocol on a 3.0T MRI scanner that can be run in under 30 minutes using novel MRI sequences. The current protocol can accommodate WS-MRI protocol in combination with WB-MRI. We believe by incorporating WB-MRI, we can provide a radiation free, fast and cost-effective technique with an improved diagnostic performance that can benefit patients by streamlining the imaging process, reducing management decision time and improving overall patients’ experience.Gains and Losses
The main challenges for WB-MR imaging are the big data sets (specifically in case of multi-parametric WB-MRI protocols) requiring improved infrastructure for data handling/viewing. Furthermore, considering its novelty, the lack of experience in WB-MR imaging amongst general radiologists might necessitate further educational and training programs. Finally, the capacity to implement WB-MRI exams on allocated ‘clinical’ time-slots on available scanner(s) might prove difficult. Conversely, the parallel developments and innovations in analyzing and viewing software packages, together with an increase in accessibility of MRI scanners might alleviate some of the current relative limitations.Acknowledgements
No acknowledgement found.References
[1] Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014; 15: e538-548.
[2] Hanrahan CJ, Christensen CR, Crim JR. Current Concepts in the Evaluation of Multiple Myeloma with MR Imaging and FDG PET/CT. Radiographics. 2010; 30: 127–142.
[3] Dimopoulos MA, Hillengass J, Usmani S, et al. Role of Magnetic Resonance Imaging in the Management of Patients With Multiple Myeloma: A Consensus Statement. J Clin Oncol. 2015; 33: 657-664.
[4] Moreau P, Attal M, Karlin L, et al. Prospective Evaluation
of MRI and PET-CT at Diagnosis and before Maintenance Therapy in Symptomatic
Patients with Multiple Myeloma Included in the IFM/DFCI 2009 Trial. Blood.
2014; 124:3359.
[5] Giles SL, deSouza NM, Collins DJ,et al. Assessing myeloma bone disease with whole-body diffusion-weighted imaging: comparison with x-ray skeletal survey by region and relationship with laboratory estimates of disease burden. Clin Radiol. 2015; 70: 614-621.
[6] Baur-Melnyk A, Buhmann S, Becker C, et al. Whole-body MRI versus whole-body MDCT for staging of multiple myeloma. Am J Roentgenol. 2008;190(4):1097–1104.
[7] Shortt CP, Gleeson TG, Breen KA, et al. Whole-Body MRI Versus PET in Assessment of Multiple Myeloma Disease Activity. Am J Roentgenol. 2009;192(4):980–986.
[8] National Institute for Health and Care Excellence (NICE) guidelines, recommendation on Myeloma diagnosis and management. https://www.nice.org.uk/guidance/ng35/chapter/recommendations#imaging-investigations
[9] Hillengass J, Fechtner K, Weber M-A, et al. Prognostic Significance of Focal Lesions in Whole-Body Magnetic Resonance Imaging in Patients With Asymptomatic Multiple Myeloma. J Clin Oncol. 2010; 28: 1606-1610.
[10] Mai EK, Hielscher T, Kloth JK, et al. A Magnetic Resonance Imaging-Based Prognostic Scoring System to Predict Outcome In Transplant-Eligible Patients With Multiple Myeloma. Haematologica. 2015; 100: 818-825.
[11] Pasoglou V, Larbi A, Collette L, et al. One-step TNM staging of high-risk prostate cancer using magnetic resonance imaging (MRI): toward an upfront simplified “all-in-one” imaging approach? Prostate. 2014;74(5):469-477.
[12] D’Sa S, Abildgaard N, Tighe J, Shaw P, Hall-Craggs M. Guidelines for the use of imaging in the management of myeloma. Br J Haematol. 2007;137: 49–63.
[13] Huang B, Wai-Ming Law M, Khong PL. Whole-Body PET/CT Scanning: Estimation of Radiation Dose and Cancer Risk. Radiology. 2009 ;251(1):166-74.
[14] Adams HJ, Kwee TC, Vermoolen MA, et al. Whole-body MRI vs. CT for staging lymphoma: patient experience. Eur J Radiol. 2014 ;83:163-6.
Figures
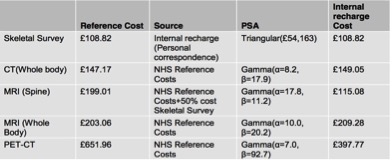
Table 1: Imaging costs (UK) used in the base case analysis and probabilistic sensitivity analysis
*: Adopted from National Collaborating Centre for Cancer document (Aug 2015). Commissioned by the National Institute for Health and Care Excellence for Consultation on diagnosis and management of multiple myeloma