4454
Can replacement sagittal diffusion images increase MR value of spinal imaging in patients with suspected malignant disease?1Centre of Medical Imaging, University College London, London, United Kingdom
Synopsis
To increase the MR value of spinal imaging in patients with suspected or known malignant disease, we propose the use of sagittal diffusion weighted imaging as replacement for traditional image types such as STIR and T2W TSE. The impact of this protocol is threefold. Scan times are reduced from potentially 50 minutes to 15 minutes for the whole spine; making scans more tolerable for patients with back pain, reducing cost and increasing scanner capacity. Reader confidence is increased in detecting malignant infiltration especially when diffuse. Finally, read times are reduced as there are fewer images to review.
Clinical Question
Can a shorter MR spine scan protocol using sagittal diffusion images as a replacement for other sequences increase MR value of spinal imaging in patients with suspected or known malignant disease?Impact
In patients with metastatic malignancy, spinal imaging may be used for diagnosis, monitoring or assessment of complications such as fractures or cord compression. Often, patients are imaged using a combination of modalities including X-rays, CT, MRI, bone scans and PET, although if there are symptoms of cord compression MRI is usually the imaging modality of choice. MRI is also used in patients with known spinal tumours to monitor response to treatment. The diagnosis of diffuse tumour infiltration can be problematic. Where there is a disease that infiltrates the entire bone marrow (such as leukaemia or advanced metastatic tumours present, for example, as may occur in Ewing’s sarcoma), the homogeneity of the marrow can mislead non-expert reporters and diffuse tumour infiltration can be missed.
Impact of revised protocol
1. Reduced scan time is of economic benefit, increases scanner capacity and is better tolerated by patients with back pain.
2. Improving confidence for diagnosing malignancy is of clinical benefit and potentially of economic benefit by reducing the use of ancillary imaging (eg PET scans).
3. Reducing scan read time is of economic benefit and increases reader capacity.
- Approach
There
is a lack of consensus on which sequences should be used as standard for 1 In our institution we use sagittal
T1W SE, sagittal T2W TSE, sagittal short tau inversion recovery (STIR), and
axial T2W TSE of the region of interest 2. A typical whole spine protocol
image acquisition time can be as long as 50 minutes. Our proposed new approach
is to use sagittal diffusion weighted imaging (TR 4000 ms, TE 65 ms, flip angle
90°, pixel bandwidth 1575 Hz, slice thickness 4 mm, b value = 800, 3 anatomical
stations) and sagittal T1W SE images
without contrast (TR 300 ms, TE 12 ms, flip angle 70°, pixel bandwidth 130 Hz, slice thickness 3 mm, 2 anatomical stations).- Gains and Losses
The gains of this approach are that acquisition time is shorter and reading time is decreased due to fewer images to review. Acquisition time for the new approach is approximately 15 minutes for the whole spine compared to 40 minutes (50 minutes with contrast) for the old approach. T1W sagittal images have been shown to be non-inferior to T2W sagittal images in detecting cord compression and superior for detecting fractures 3,4. Therefore in terms of diagnostic information we expect non-inferiority compared to the traditional approach. DWI may be more specific for tumour and tumour response than STIR imaging 5, and diffuse malignant disease should be more easily detectable on DWI than conventional imaging.
The main losses of this approach are the lack of axial images and the potential for missing malignant pathology through the use of fewer sequences. However the new approach does not preclude the use of additional sequences on a case-by-case basis if the new 2-sequence protocol is not sufficient. We hypothesise that malignant lesions are at least as conspicuous on DWI as STIR. It is foreseeable that benign cause of back pain in these patients may not be apparent on the new approach such as disc protrusions.
- Preliminary Data
Our preliminary retrospective data are derived from an experimental protocol including all the above mentioned traditional sequences with the addition of sagittal diffusion sequence on 10 patients with known malignancies including multiple myeloma, gastric, breast and rectal cancer. Representative areas of malignant infiltration are highlighted by arrows on the DWI image. The diagnostic information gleaned from the high value protocol was equivalent to the old protocol. Diffuse infiltration was better demonstrated by DWI compared to STIR (Figure 4). The T1W images were sufficient as an anatomical sequence compared to T2W images.
We predict that a whole spine protocol consisting of sagittal DWI and unenhanced sagittal T1W spin echo would take approximately 15 minutes compared to the traditional approach and thus reduce costs per patient, and increase patient throughput. Cost effectiveness would also be increased shorter scan reading times. Furthermore a shorter scan time will improve patient experience especially those with severe back pain.
Acknowledgements
No acknowledgement found.References
1. Wang B, Fintelmann FJ, Kamath RS, Kattapuram S V, Rosenthal DI. Limited magnetic resonance imaging of the lumbar spine has high sensitivity for detection of acute fractures, infection, and malignancy. Skeletal Radiol. 2016
2. Shah LM, Salzman KL. Imaging of spinal metastatic disease. Int J Surg Oncol. 2011;2011:769753
3. Johnson AJ, Ying J, El Gammal T, Timmerman RD, Kim RY, Littenberg B. Which MR imaging sequences are necessary in determining the need for radiation therapy for cord compression? A prospective study. AJNR Am J Neuroradiol. 2007;28(1):32–37
4. Kim JK, Learch TJ, Colletti PM, Lee JW, Tran SD, Terk MR. Diagnosis of vertebral metastasis, epidural metastasis, and malignant spinal cord compression: are T(1)-weighted sagittal images sufficient? Magn Reson Imaging. 2000;18(7):819–824
5. Lecouvet FE, Larbi A, Pasoglou V, et al. MRI for response assessment in metastatic bone disease. Eur Radiol. 2013;23(7):1986–1997
Figures
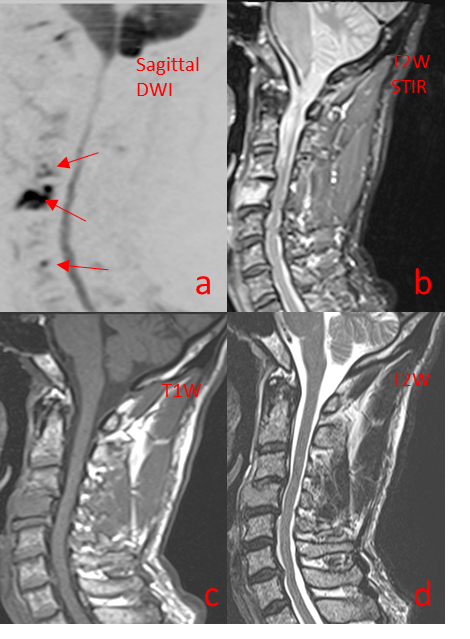
Figure 1
Sagittal MR images of the cervical spine of a patient with Multiple Myeloma 1a = sagittal DWI, 1b = T2W STIR, 1c = T1W, 1d = T2W (Old approach = b+c+d; New approach = a+c)
1a demonstrates restricted diffusion in the brain, spinal cord and focal areas in C3, C4 and C6 (arrows) in keeping with malignant infiltration. No further diagnostic information is obtained from the conventional protocol images (b+c+d) when compared to the new value protocol (a+c). Acquisition time for the old protocol images (b+c+d) was 9 minutes versus 4 mins for the new protocol (a+c) images.
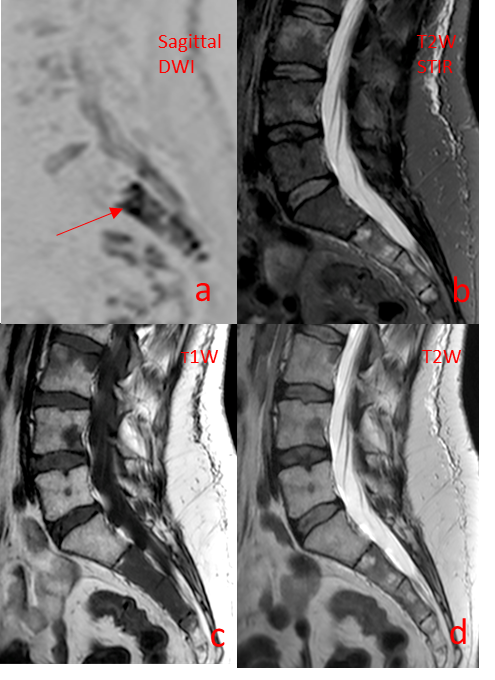
Figure 2
Sagittal MR images of the lumbar spine of a patient with metastatic breast cancer
2a = sagittal DWI, 2b = T2W STIR, 2c = T1W, 2d = T2W
(Old approach = b+c+d; New approach = a+c)
2a demonstrates focal areas of restricted diffusion in L4, S2 (arrow) and further areas in S3, S4 in keeping with malignant infiltration. No fractures are demonstrated on T1W images (2c). No further diagnostic information is obtained from the conventional protocol images (b+c+d) when compared to the new value protocol (a+c). Acquisition time for b+c+d was 8 minutes and for a+c, 3 minutes.

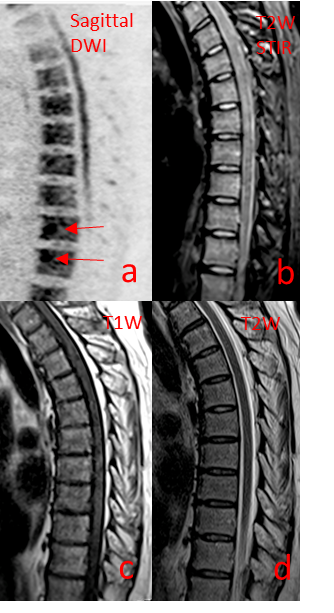
Thoracic spine sagittal MR images of a patient with Multiple Myeloma
3a = sagittal DWI, 3b = T2W STIR, 3c = T1W, 3d = T2W
(Old approach = b+c+d; New approach = a+c)
3a demonstrates focal areas of restricted diffusion in two thoracic vertebrae (arrows) in keeping with malignant infiltration. No fractures are demonstrated on T1W images (3c). No further diagnostic information is obtained from the conventional protocol images (b+c+d) when compared to the new value protocol (a+c). Acquisition time for b+c+d images was 9 minutes and for a+c was 4 minutes.
Thoracic spine sagittal MR images of a patient with Multiple Myeloma
4a = sagittal DWI, 4b = T2W STIR, 4c = T1W, 4d = T2W
(Old approach = b+c+d; New approach = a+c)
4a demonstrates diffuse areas of restricted diffusion in multiple thoracic vertebrae; more focal areas are highlighted in two thoracic vertebrae (arrows). Diffuse involvement is more apparent on DWI (4a) versus STIR (4b). No further diagnostic information is obtained from the conventional protocol images (b+c+d) when compared to the new value protocol (a+c). Acquisition time for b+c+d images was 9 minutes and for a+c was 4 minutes.