4448
Robust high‑throughput Cardiac MR featuring Compressed Sensing1Siemens Healthcare, Erlangen, Germany, 2Siemens Healthcare Ltd, Frimley, Surrey, United Kingdom, 3Department of Radiology, Royal Bournemouth Hospital, Bournemouth, United Kingdom
Synopsis
A standard CMR protocol for the evaluation of cardiac function and myocardial damage in patients with ischemic or non-ischemic heart-disease was compared to a new approach which drastically reduces the scan time. This was achieved by introducing a highly accelerated compressed sensing cine sequence which facilitated significant work-flow optimization. Image quality scores of both methods were equivalent and quantitative results showed good agreement. The mean examination time was reduced from 26:29 ± 5:45 min to 16:15 ± 2:47 min, which corresponds to a 38 % reduction in examination time.
Clinical Question
To assess cardiac function and myocardial damage in patients with ischemic or non-ischemic heart disease using highly accelerated MR image acquisition techniques combined with an easy‑to‑use and cost‑effective workflow.
Impact
Heart failure is a major global cause of morbidity and mortality, with anticipated increase in prevalence in the next decade1. Both cardiovascular MR (CMR)-based measurements of left and right ventricular ejection fraction as well as late-Gadolinium enhancement (LGE) have been shown to be good predictors of prognosis in both ischemic and non-ischemic heart disease2. Clinical limitations of CMR include lack of expertise and availability, costs, as well as reduced reliability in patients with dyspnea or irregular heart rates. The costs of a CMR examination could be markedly reduced and the patient population increased by reducing overall examination time through the use of faster imaging techniques.
Approach
In this work, we compare a standard CMR examination for the evaluation of cardiac function and myocardial damage, with a new, faster approach that drastically reduces the overall scan duration. Both examinations, which are shown graphically in Figure 1, were performed using the Cardiac Dot Engine (Siemens Healthcare, Erlangen, Germany). This software allows for workflow standardization, reduction in complexity as well as an overall shorter examination3. The standard workflow includes localization, ‘whole thorax surveys’ and long-axis CINEs, all of which are performed prior to contrast agent administration. After the administration of a Gadolinium-based contrast agent (GBCA), short-axis cines with whole ventricle coverage were performed for the assessment of function and mass. These were followed by aortic flow quantification and LGE imaging in the short- and long-axis heart orientations around 10 minutes after GBCA injection.
The new, high value protocol combines highly accelerated compressed sensing cine (CS CINE) with a re-optimized workflow which involves administrating contrast media at the start of the examination. The benefits of this approach are two-fold. First of all the entire examination is shorter since cine imaging for left ventricular function analysis can be performed in a markedly reduced number of breath-holds, whilst still allowing for LGE imaging 10 minutes post-contrast, as per recommendations. The CS CINE prototype is a real-time sequence with temporal and spatial resolution comparable with that used conventionally. Table 1 compares the parameters of both the conventional and highly accelerated cine methods. Prior work has shown that quantitative parameters of LV function are comparable for both methods, with significant time saving4. Second of all, CS CINE, being a real-time method, can potentially reduce the variability in image quality due to arrhythmia or dyspnea since data acquisition is performed within single heartbeats.
Forty‑one patients were examined with the traditional approach and 32 patients with the novel approach. In 13 of the patients scanned with the new method, standard short-axis CINEs were also obtained at the end of the examination for qualitative and quantitative comparison purposes. Image quality, breath-hold compliance and ECG regularity were scored using a 5-point Likert scale (1 for poor, 5 excellent). The study was performed on a commercially available MR system (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany).
Gains and Losses
The innovative protocol significantly reduces the total “table” time, which in turn allows for an increase in patient throughput, as shown in Table 2, and a reduction in the total examination costs. A potential disadvantage is the fact that all acquisitions are performed post-contrast, thus limiting the imaging options available in the case of incidental findings.
Preliminary Data
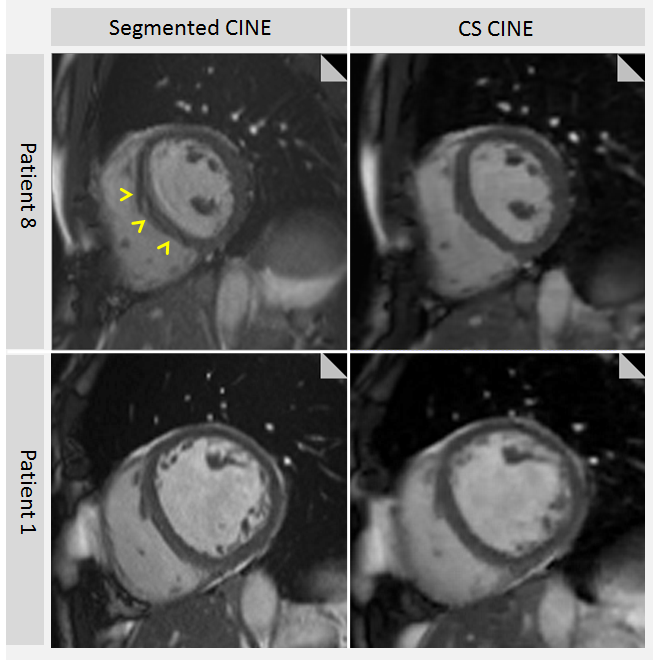
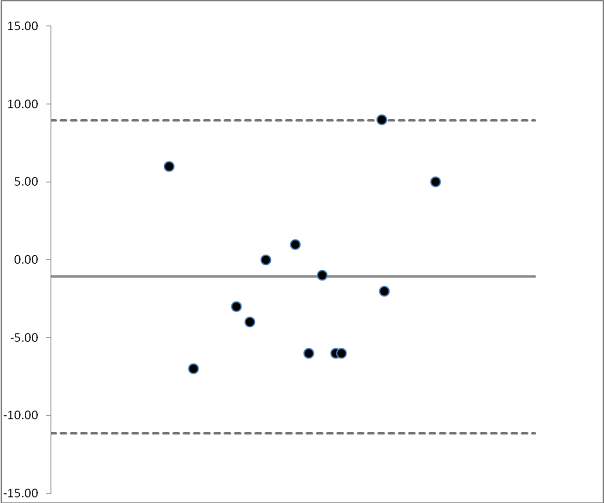
The mean image quality score for both methods was equivalent (4.20 ± 0.91 conventional versus 4.12 ± 0.49 for compressed sensing). In the two cases where the image quality of CS cine scored < 4 this was due to artifacts originating from inhomogeneous regions. With the conventional approach, 12 different patient datasets got an image quality score < 4, all of which also scored low on ECG regularity and/or breath-holding. The real-time CS CINE was more robust in patients with ECG irregularities and poor breath-hold compliance (Figure 2). In the compliant subjects image quality was scored slightly higher for the conventional method. This is likely attributable to the reduction in the sharpness of the blood-myocardial boundaries as a consequence of high degree of sub‑sampling (Figure 2). Nevertheless, quantitative results are comparable with both methods as shown in the Bland-Altman plot in Figure 3, which compares the ejection fractions determined from the conventional and the innovative MR imaging protocols.
Acknowledgements
No acknowledgement found.References
1. D Mozaffarian, et al. Executive Summary: Heart Disease and Stroke Statistics--2016 Update: A Report From the American Heart Association. Circulation. 2016 Jan 26;133(4):447-54
2. T D Karamitsos, et al. The Role of Cardiovascular Magnetic Resonance Imaging in Heart Failure. JACC Vol. 54, No. 15, 2009
3. S J Thomas, et al. The need for speed - adenosine stress MRI in less than 30 minutes. JCMR. 2013; 15 (Suppl 1):E24.
4. Kido T, et al. Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold. JCMR. 2016 Aug 24;18(1):50
Figures
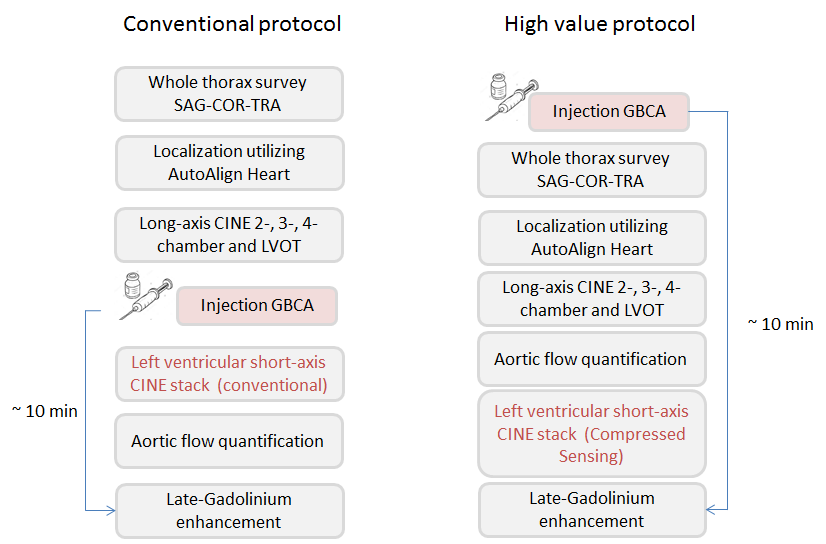
Figure 1: Conventional protocol with injection of GBCA in the middle of the examination, compared with the high value CS CINE protocol with injection of GBCA right at the start of the examination.
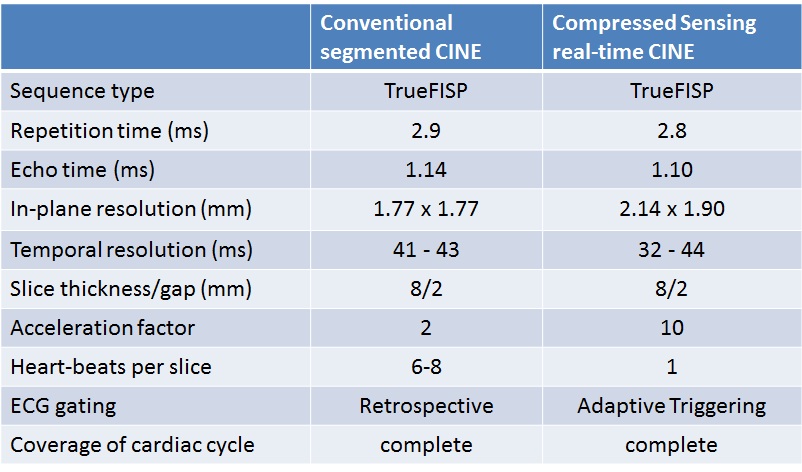
Table 1: Protocol parameters for the conventional segmented CINE compared to the CS CINE. Adaptive Triggering, used for CS CINE reacts, in real-time, to the detected triggers.
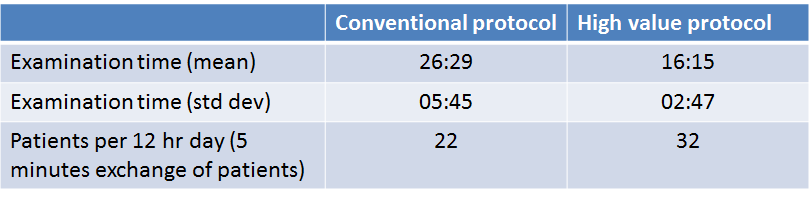
Table 2: Mean examination time and standard deviation, calculated from first acquired to the last reconstructed image for the conventional protocol compared to the high value protocol. Patient throughput calculated for a 12 hour working day, including 5 minutes for exchange of patients for both protocols.