4447
Increasing value of MRI in evaluation of gynecologic malignancies by decreasing scan time and reducing artifacts through the replacement of fast spin echo (FSE) with variable refocusing flip angle single-shot FSE (vrfSSFSE)1Radiology, Stanford University, Stanford, CA, United States, 2Global MR Applications and Workflow, GE Healthcare
Synopsis
Variable refocusing flip angle single-shot fast spin echo (vrfSSFSE) with outer volume suppression (OVS) improves upon standard single-shot fast spin echo (SSFSE or HASTE): 1) decreasing average flip angles thereby reducing specific absorption rate (SAR) limited acquisition times, 2) reducing blurring from T2 decay, 3) allowing full-Fourier acquisitions. Although improving upon conventional SSFSE, it remains unknown if vrfSSFSE with OVS can approach the image quality and diagnostic capability of fast spin echo (FSE). We found vrfSSFSE comparable to FSE in signal-to-noise and contrast and superior to FSE in coherent artifact reduction, depending on the plane of imaging.
Clinical Question
Can variable refocusing flip angle single-shot fast spin echo (vrfSSFSE) with outer volume suppression (OVS) increase the value of MRI in the setting of gynecologic malignancy, by providing more time efficient and superior T2-weighting imaging (T2WI) in comparison to fast spin echo (FSE)?Impact
MRI of the pelvis performed for staging of uterine and cervical malignancies is heavily reliant on T2WI for accurate assessment of the presence and extent tumor. Clinical and surgical management are directly impacted by these findings, while degradation of image quality undermines clinical confidence. When a noninvasive assessment like MRI fails to optimally characterize the disease, surgical and psychosocial implications for the patient are by no means insignificant, given that the primary intervention is hysterectomy.
Image quality commonly suffers from long scan times associated with FSE-based T2WI, which cause bowel peristalsis and respiratory motion to degrade the acquisition. Diminishing scan time is vital for minimizing coherent artifacts, which in turn maximizes diagnostic capability and improves the clinical impact of MRI. Additionally, relatively long acquisition times required by FSE-based T2WI leads to longer total exam times, limiting availability of MRI in scanner constrained environments and increasing per study cost.
Approach
T2WI of the pelvis is currently performed using FSE. Attempts to lessen acquisition times have integrated fast recovery into FSE. Single-shot FSE (SSFSE or HASTE) can further reduce scan times, helping to reduce motion artifacts. SSFSE is accomplished through implementation of a long refocusing pulse train and half-Fourier acquisition, where all necessary data points in k-space are obtained within one repetition time. However, SSFSE falls short in comparison to FSE because of an inferior signal-to-noise ratio (SNR) and limited effective resolution due to T2 blurring. Furthermore, scan times for SSFSE can be artificially prolonged, especially at 3T, due to specific absorption rate (SAR) limitations that arise from the long train of high flip angle refocusing pulses.
An alternate technique, called vrfSSFSE, decreases and varies the refocusing flip angle over the single-shot acquisition, decreasing energy deposition and mitigating T2 decay related blurring.1 This technique improves image quality and perceived diagnostic capability over SSFSE.2 By combining vrfSSFSE with OVS, fewer phase-encoding steps are required, allowing full-Fourier acquisition with clinically relevant effective echo times.3 Therefore, our study design included independent assessments of vrfSSFSE with OVS and FSE (image quality metrics, lesion detection, diagnostic confidence) as well as blinded side-by-side evaluations of reader preference using appropriate nonparametric, paired assessments.
Gains and Losses
Through prior research, vrfSSFSE has been optimized and is clinically available for body MRI interpretation at several institutions including our own. With this early success, we hypothesized that vrfSSFSE with OVS would improve image quality and diagnostic ability over FSE in the setting of gynecologic malignancy. Additionally, we hypothesized reader preference for vrfSSFSE.
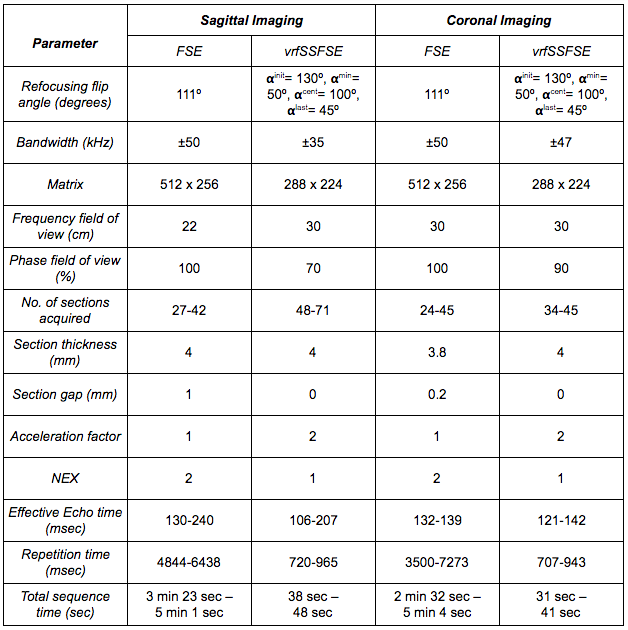
This was an IRB-approved, HIPAA-compliant retrospective study of pelvic MRI exams that included both coronal and sagittal FSE and coronal and sagittal vrfSSFSE with OVS (Table 1). In this way, initial implementation of vrfSSFSE entailed no potential loss of current clinical diagnostic accuracy. Additionally, the downside of additional sequences was limited, adding slightly more than a minute of scan time from coronal and sagittal vrfSSFSE sequences combined. The cohort was limited to the clinical indication of uterine and cervical malignancy.4,5
Preliminary Data
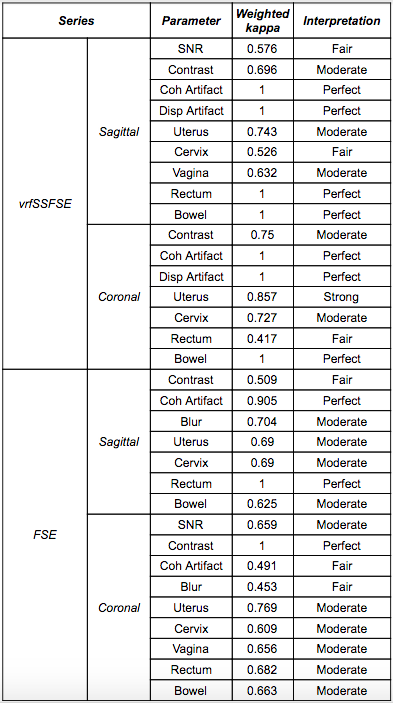
This preliminary assessment represents the challenging comparison between FSE versus vrfSSFSE in the case study of gynecologic malignancy. Among a cohort of 14 patients, average patient age was 52.7 ± 19.4 years. Inter-reader agreement was moderate or better for the majority of metrics (Table 2).
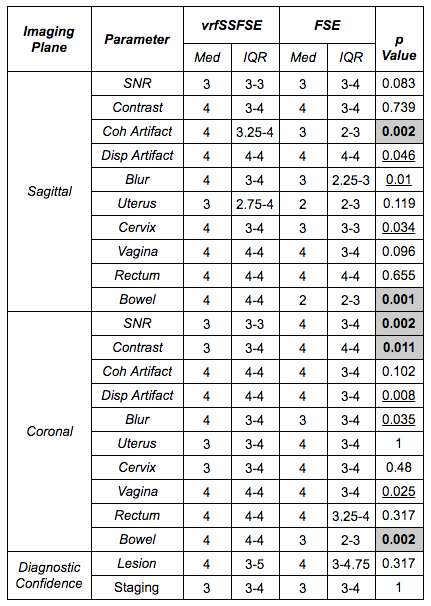
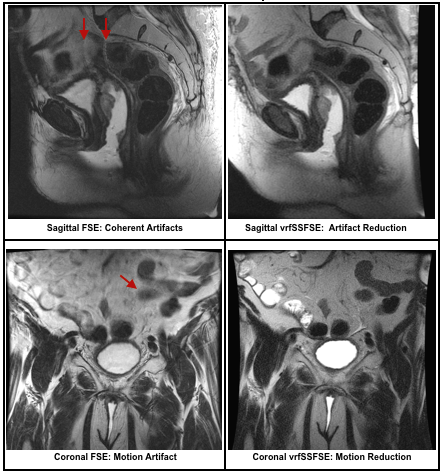
Usually plagued by motion degradation, sagittal T2WI demonstrated significant improvement (less coherent motion artifacts) on vrfSSFSE (Fig. 1). Sagittal vrfSSFSE manifested no significant difference in SNR or image contrast in comparison to FSE, demonstrating remarkable robustness of vrfSSFSE with OVS as an acquisition taking less than 20% of the time as FSE (Table 3). This temporal efficiency will translate into cost-efficiency as vrfSSFSE should be a replacement rather than addition to current acquisitions, thereby resulting in time and potentially cost savings through improved throughput. However, coronal vrfSSFSE was clearly inferior to FSE.
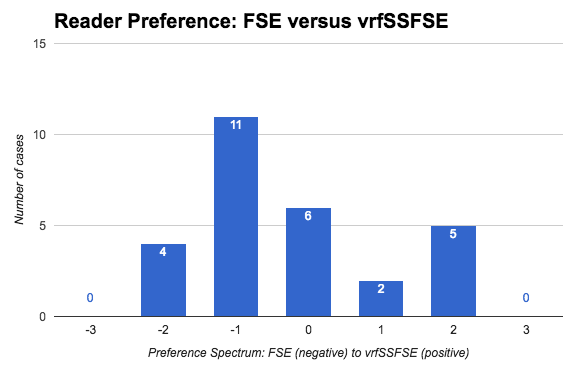
Readers were equally confident in lesion detection and staging for both T2WI techniques; no significant difference in preference was detected (p = 0.450) (Fig. 2). Importantly, frequency of lesion detection did not differ (p = 1.0).
Interchangeability of vrfSSFSE with FSE is not a trivial realization considering the rapidity of vrfSSFSE. This efficiency lends itself well to the pelvis, where interrogation of curvilinear pelvic organs often necessitates multiple obliquities for optimal assessment.
Acknowledgements
This work was in part supported by NIH grant R01 EB009690. The authors would also like to thank the support of GE Healthcare.References
1. Loening AM, Saranathan M, Ruangwattanapaisarn N, Litwiller DV, Shimakawa A, Vasanawala SS. Increasing speed and image quality in single-shot fast spin echo imaging via variable refocusing flip angles. J Magn Reson Imaging. 2015;42:1747-1758.
2. Loening AM, Litwiller DV, Saranathan M, Vasanawala SS. Increased speed and image quality for pelvic single-shot fast spin-echo imaging with variable refocusing flip angles and full-Fourier acquisition. Radiology. 2017;000:1-8. [Epub ahead of print]
3. Taviani V, Litwiller D, Loening AM, Saranathan M, Hargreaves BA, Vasanawala SS. Single-shot fast spin echo of targeted regions with variable refocusing flip angles and quadratic phase pulses for outer volume suppression. Proc Intl Soc Magn Reson Med. 2015. Abstract ID 0948.
4. Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103-104.
5. Kohorn EI. The new FIGO 2000 staging and risk factor scoring system for gestational trophoblastic disease: description and critical assessment. Int J Gynecol Cancer. 2001;11:73-77.
Figures