4378
Application of dynamic contrast-enhanced MRI in differential diagnosis of benign and malignant lung lesions1Department of Radiology, First People’s Hospital of Yangzhou, Yangzhou, People's Republic of China, 2MR Research China, GE Healthcare, Shanghai, People's Republic of China, 3GE Healthcare
Synopsis
Dynamic contrast enhancement (DCE) MRI is rarely used in lung lesions in previous studies, because of the influence of heart rate and respiratory motion. With the development of 3D non-rigid registration algorithm, high resolution dynamic enhanced MRI application in lung disease is increasing. After registration, the image is more clearer and the quantitative parameters are more accurate. The quantitative parameters Ktrans and Kep are capable of differentiating benign and malignant lung lesions, which has an important value in clinical work.
Objectives
Lung cancer is one of the most common malignant tumors. The incidence and mortality of lung cancer ranks first among all the malignant tumors [1]. Chest X-ray and CT scanning used to be routine examination for lung tumor [2], but it is difficult to differentiate benign and malignant lung tumor by morphological changes. Magnetic resonance imaging has the advantage of better soft tissue contrast, no ionizing radiation, and capability of providing angiogenesis related functional information. Due to the influence of heart rate and respiratory motion, dynamic contrast enhancement (DCE) MRI is rarely used in previous studies. With the development of 3D non-rigid registration algorithm, high resolution dynamic enhanced MRI application in lung disease is increasing [3]. This study aims to calculate quantitative permeability related parameters and explore its clinical value in differentiating between benign and malignant lung lesions.Methods
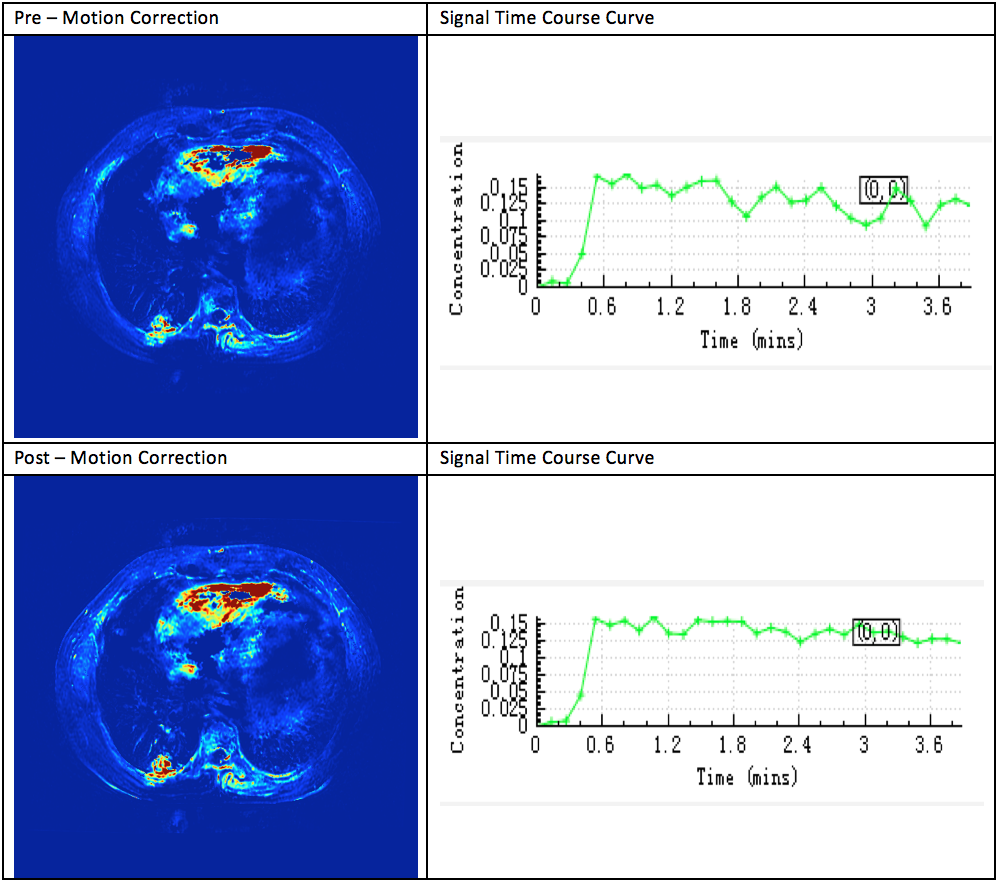
Twenty-five patients (11 women, 14 men, median age 63, age range 40-75) diagnosed with pulmonary lesion underwent routine MR exams and DCE MRI on a 3.0T whole body system (GE Discovery 750W) equipped with 16 channel surface coil. Among these patients, 17 patients had lung cancer and 8 patients had benign pulmonary nodules. The DCE prescription were performed as follows: 3D T1 weighted gradient echo sequence with five different flip angles (3° to 15°, in step of 3°) were acquired prior to dynamic scan for T1 mapping. In dynamic scan, 40 phases were acquired with time resolution of 7s. Gadodiamide (0.1 mmol/kg, Omniscan, GE Healthcare) was intravenously injected by power injector after the first two phases. Multiple flip angle and multiphase acquisitions were processed using a commercial DCE post processing software (Omni-Kinetics). Non-rigid 3D registration (Fig.1) was carried out prior to two chamber deconvolution with standard Tofts model. The arterial input function (AIF) were sampled from normal thoracic aorta. The following permeability parameters were calculated: volume transfer constant Ktrans, return rate constant rate constant Kep, extravascular extracellular volume fraction Ve, and blood plasma volume Vp. The ROI placement principles are: (1) determined by 2 senior radiologists; (2) ROI placed in the most enhanced areas (refer to conventional T2WI and image enhancement); (3) avoid vascular necrosis, liquefaction and artifacts; (4) manual delineation of ROI; (5) the area is 25 mm2; and (6) measure both the center of the lesion and the adjacent level two levels once and take the average value of the 3 measurements.Results
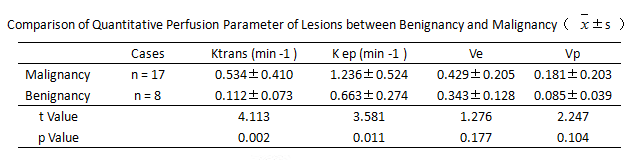
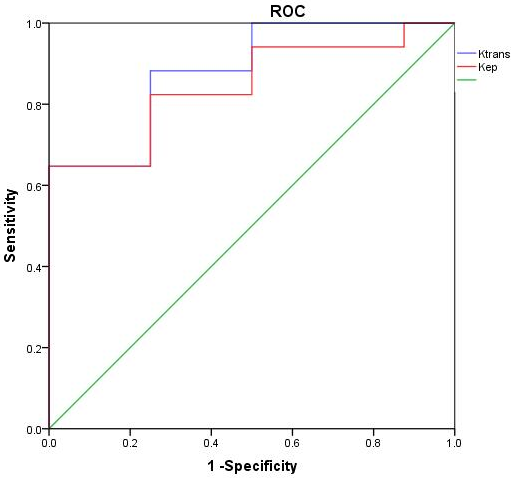
The mean Ktrans, Kep, Ve, and Vp of malignant and benigh lesions were listed in Table.1. There were significant differences between malignant lesions and benign lesions in Ktrans and Kep (t=4.113, 3.581, respectively, P<0.05). No significant differences were found between malignant and benign lesions in Ve and Vp (t=1.276, 2.247, respectively, P>0.05). The area under the ROC curve (AUC) of Ktrans and Kep for malignant and benign lesions were 0.882 and 0.846 respectively Fig.2. The sensitivity of these five parameters were 92.3% and 91.7%, and specificity were 87.5% and 75.0% for the differentiating pulmonary lesion if using the maximum Youden index as cut-off.Conclusion
The DCE-MRI can quantitatively evaluate the microvascular permeability. The quantitative parameters Ktrans and Kep are capable of differentiating benign and malignant lung lesions, which has an important value in clinical work.Acknowledgements
No acknowledgement found.References
[1] Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014;64(1):9–29.
[2] Ohno Y, Nishio M, Koyama H, et al. Dynamic contrast-enhanced CT and MRI for pulmonary nodule assessment[J].AJR Am J Roentgenol, 2014, 202(3):515-529.
[3] YM Mei, MD Yu-Dong Zhang, ZM Chan, et al. Comparison of intravoxel incoherent motion diffusion-weighted MR imaging with dynamic contrast-enhanced MRI for differentiating lung cancer from benign solitary pulmonary lesions[J]. Journal of Magnetic Resonance Imaging Jmri, 2016,43(3):669-679.
Figures