4372
Rapid MR Pancreatic and Ovarian Screening Imaging for Patients with BRCA Mutation Undergoing Screening Breast MRI – Pilot Study1MSKCC, New York, NY, United States
Synopsis
The purpose of this study was to develop and optimize a rapid MR pancreas and ovarian screening protocol to be performed in conjunction with breast MRI screening in BRCA mutation carriers. Images were acquired with the patient in the prone position, with the breast coil still in place, but using the built-in body coil on a 3T magnet, and evaluated for image quality and detection of lesions. 30 women had research MR for pancreatic screening and 5 of them also underwent for rapid ovarian MR screening which provided diagnostic quality images within a short time of acquisition.
Purpose
BRCA 1 and 2 mutations carriers are at a greater risk of developing breast, ovarian, and pancreatic cancer. Annual magnetic resonance imaging (MRI) starting at age 25 years is recommended for women with a known BRCA mutation. Although no specific screening guidelines exist for ovarian and pancreatic cancer in this population, individualized screening approaches should be considered (1). As these patients are already undergoing MRI screening on a regular basis, this potentially allows for incorporation screening of other at risk organ systems at the same time. The purpose of this study was to create and optimize a rapid pancreatic and ovarian MR screening protocol that could be used in conjunction with breast MRI screening in BRCA-positive individuals.Methods
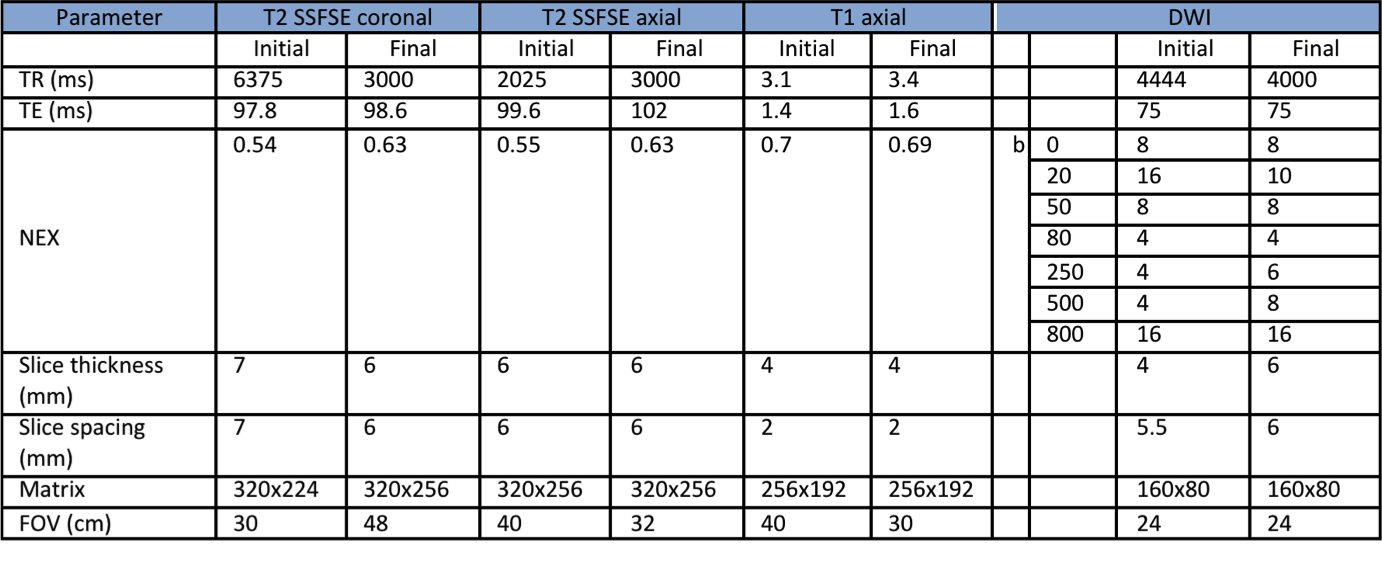
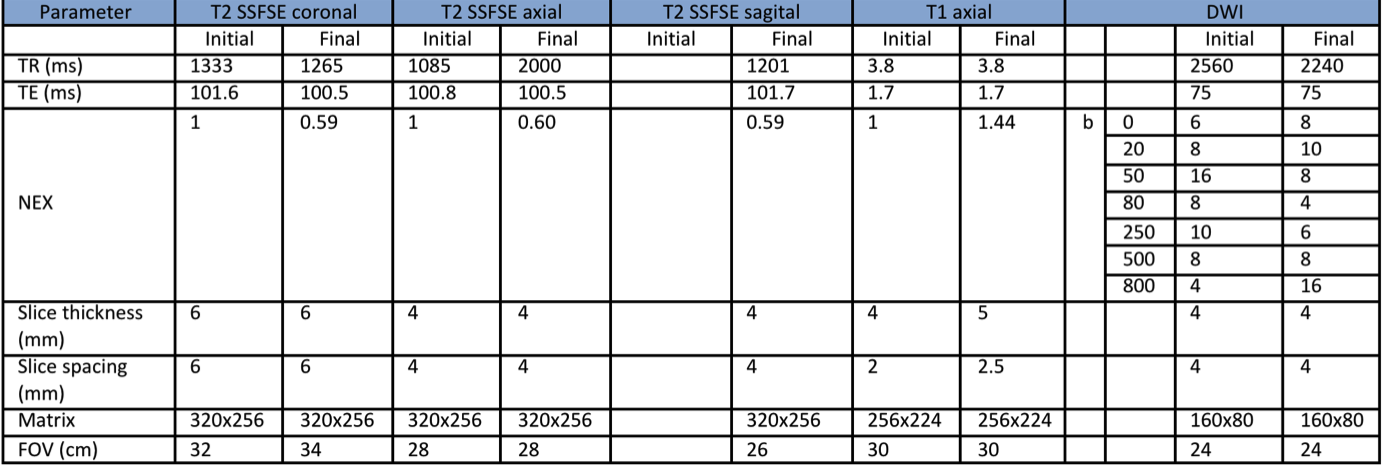
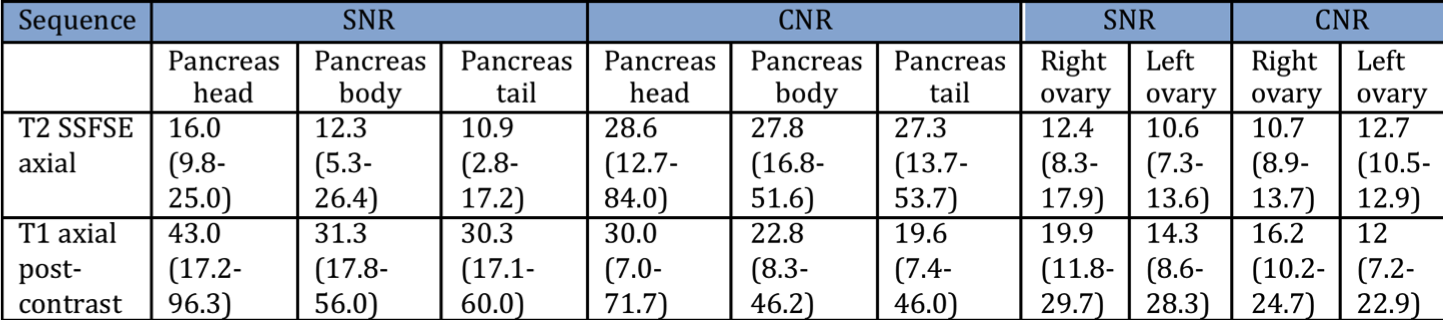
In this prospective cohort study, BRCA 1 or 2 mutation women carriers attending for their scheduled screening breast MRI were eligible to participate. The local IRB approved the HIPPA compliant protocol, written informed consent was obtained. Women participating had screening Breast MRI as per routine. Additionally, research MR screening was done. The rapid screening protocol was designed to be completed in less than 15 minutes at the completion of the breast MRI. The images were acquired using the built-in body coil without placement of a dedicated body surface coil, with the patient still in the prone position, and the breast coil in place. Sequences performed included T2 SSFSE, T1 axial post-contrast, and reduced field of view (rFOV) DWI. All studies were performed on a 3T GE magnet. The primary objective was to define an optimize MRI acquisition. Subjective and objective measures of image quality were assessed by two radiologists. First, overall image quality was assessed on a 5-point scale (1 = all diagnostic information present, 5 = non-diagnostic). The imaging protocol was modified until diagnostic images were achieved for 5 consecutive patients, at which point the protocol was considered optimized. Images were also reviewed by the same two diagnostic radiologists in consensus for detection of pancreatic and ovarian lesions. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were assessed by manually placing regions-of-interest (ROI) with 8 mm diameter in the pancreas, and with 3 mm in ovaries and the adjacent fat determining the mean signal intensity (S). A further ROI was placed over the background air according to the following equations: $$SNR = \frac {Stissue}{SD_{air}}$$$$CNR = \frac {Stissue-Sfat}{SD_{air}}$$As not all sequences included background air, SNR to be calculated using subtraction methods (3). Results
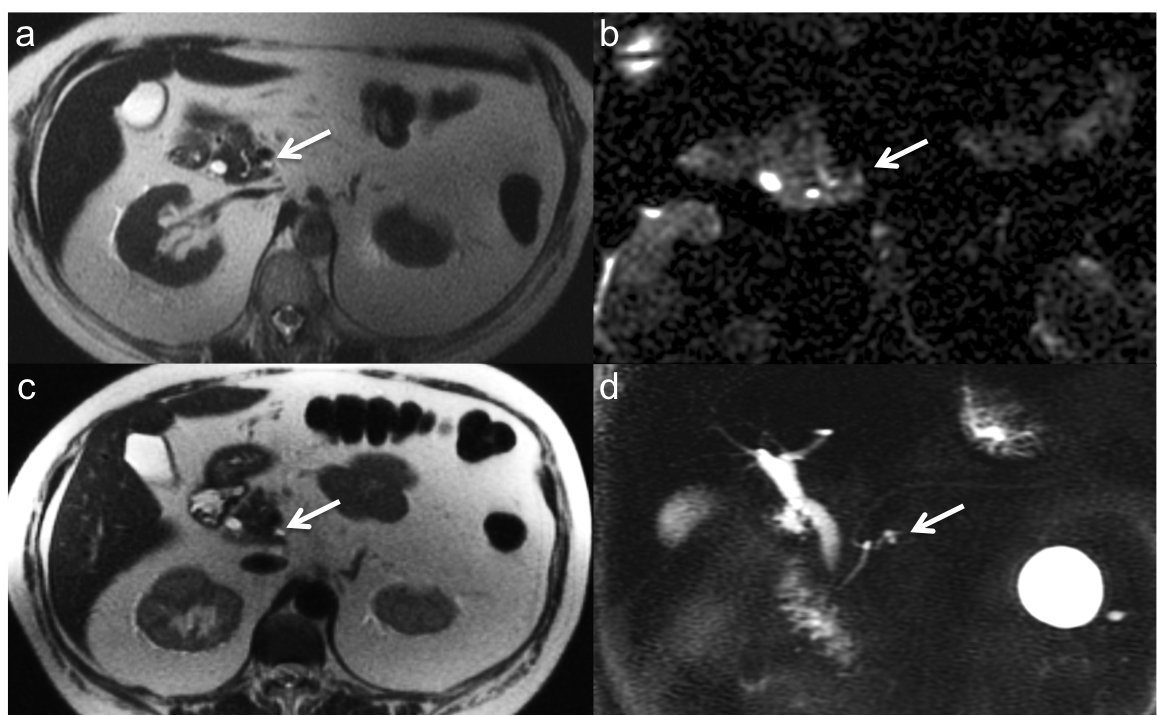
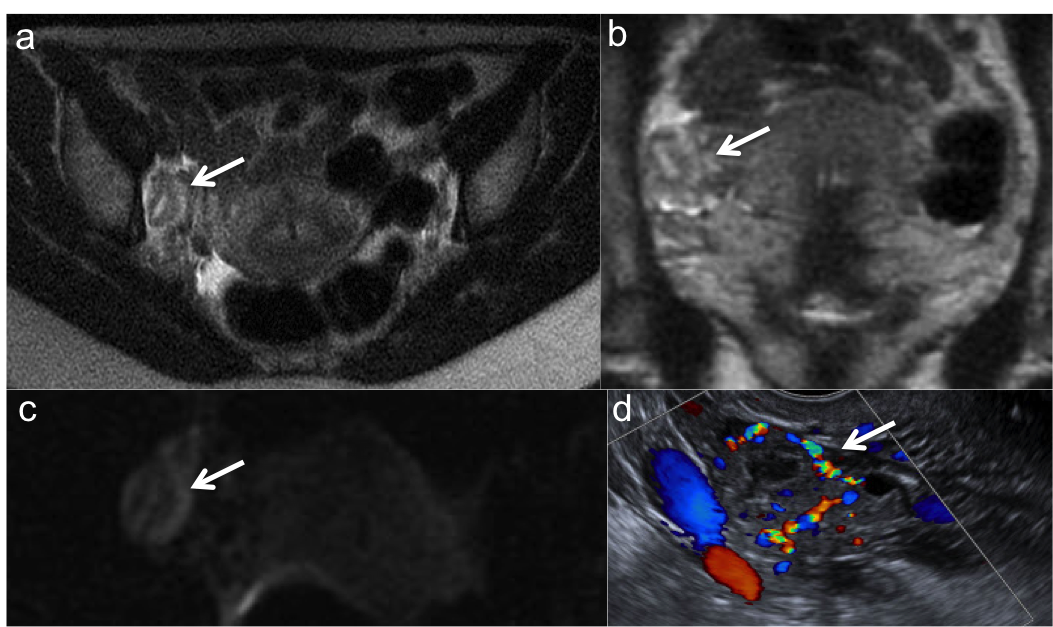
Between July 2015 and October 2016, 30 BRCA-positive women had research MR for pancreatic screening and 5 also underwent rapid ovarian MR screening protocol at the conclusion of their breast MRI. The MR research protocol was successfully completed in all patients. Following subject 1, for the pancreas protocol parameters for axial T1-post-contrast and rFOV DWI were modified to improve image quality (Table 1) and for the ovarian protocol T1 axial weighted image was modified after subject 3 (Table 2). Average time for the pancreatic protocol was 9:24 and for the ovary was 3:62 m:s. Excellent image quality was achieved after the protocols were modified for all patients for the T2 SSFSE, and T1 weighted sequences. SNR and CNR values are reported in Table 3 (Table 3). In 4 patients, small pancreatic cystic lesions were detected (Figure 1) and 2 patients presented ovarian benign findings (cospus luteum) (Figure 2). Discussion
Our study demonstrates that rapid MR pancreatic and ovarian cancer screening imaging is feasible and yields diagnostic image quality. For the higher b-values of 500 and 800 s/mm2 the lower SNR obtained accounted for the subjectively lower image quality scores assigned. In the final version of the protocol we plan to use 3 b-values (0, 50, and 500 s/mm). The prevalence of pancreatic lesions (13%) observed in our study is within the reported range in high risk individuals(3). Combined with breast MRI screening, this protocol may allow for earlier detection of malignant or pre-malignant lesions, potentially reducing the cost and the stress to the patient by decreasing the number of separate screening examinations performed. This study was not designed to assess the effectiveness of pancreatic or ovarian cancer screening itself, but rather to develop a comprehensive screening tool that can be performed in a limited time frame at the conclusion of a breast MRI, and that could eventually be further evaluated in larger clinical trials. Conclusion
Rapid MR protocol for pancreatic and ovarian cancer screening with subjects in the prone position and use of the built-in-body coil is feasible and provides diagnostic quality images.Acknowledgements
No acknowledgement found.References
1. Daly MB, Pilarski R, Berry M, et al. NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 1.2017. Fort Washington, PA: National Comprehensive Cancer Network; 2016.
2. NEMA Standards Publication MS 1-2008 (R2014). Determination of Signal-to-Noise Ratio (SNR) in Diagnostic Magnetic Resonance Imaging. Rosslyn, Virginia: National Electronical Manufacterers Association; 2008.
3. Canto M, Hruban R, Fishman E, et al. Frequent detection of pancreatic lesions in asymptomatic high-risk individuals. Gastroenterology. 2012; 142(4):796-804.
Figures