4310
Lightweight Size Optimized Printed Pediatric Receive Array1UC Berkeley, Berkeley, CA, United States, 2Stanford Hospital
Synopsis
The current landscape of pediatric body MRI lacks dedicated high-density arrays, especially for small children. Therefore many centers use existing arrays designed for adults. These arrays are much larger than the patients, reducing the effective number of elements. Adult arrays are heavy for children and are supported by additional padding, increasing the distance from the patient and reducing image quality. Here, we present an appropriately sized blanket-like array designed from patient data for torso and chest/abdominal imaging of 0-2 and 3-5 year olds respectively. This pediatric array is fabricated using screen-printed electronics to produce an extremely lightweight and flexible coil.
Introduction
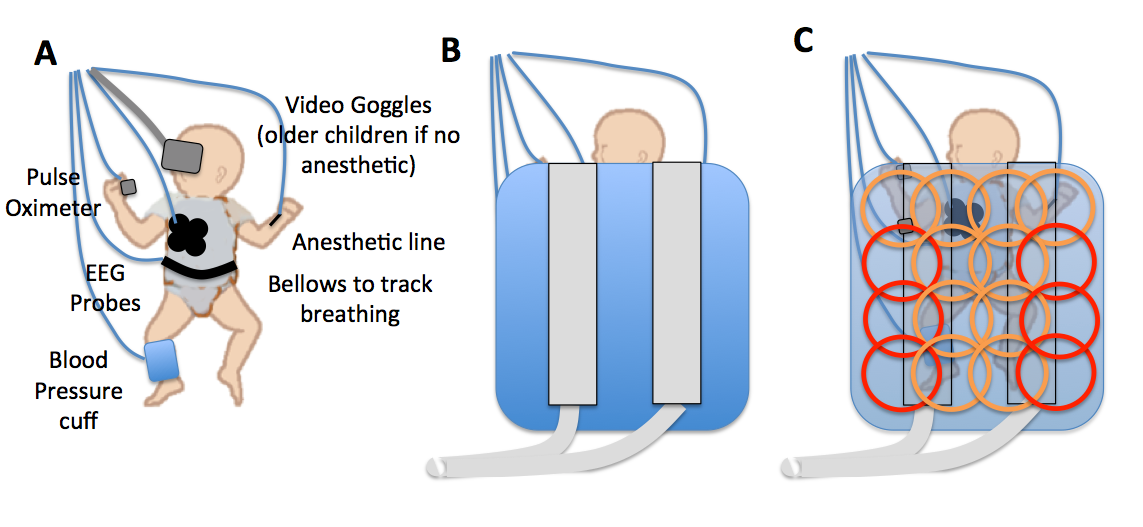
The practice in many pediatric MRI institutions is to perform scans using existing high-density receive coils intended for adults. For example, it is common for an adult cardiac array to be used for chest or abdominal pediatric imaging. These arrays do not fit the patients well and are relatively heavy, at times weighing more than patient. The weight of the arrays can compress the patient and impede breathing. Pediatric patients also have other sensing or drug delivery hardware attached, adding to the overall weight worsening the problem – Fig 1 A. Technologists can offset the array using a plastic former or even rolled-up towels, but this moves the array further away from the patient, introducing a performance-reducing gap. Additionally, several of the array elements are usually not close enough to the patient to contribute any useful signal – Fig 1 B and C. Previous works introduced better-suited array designs for pediatric patients [1, 2], but relied on traditional means of fabrication.
In this work, we improved upon earlier designs by using printed electronics techniques to produce extremely lightweight, flexible, and customizable receive arrays [3, 4]. We collected and used image data from a children’s hospital to make an array optimized for pediatric patients. The lightweight arrays were then used to image several phantoms and a volunteer.
Methods and Discussion
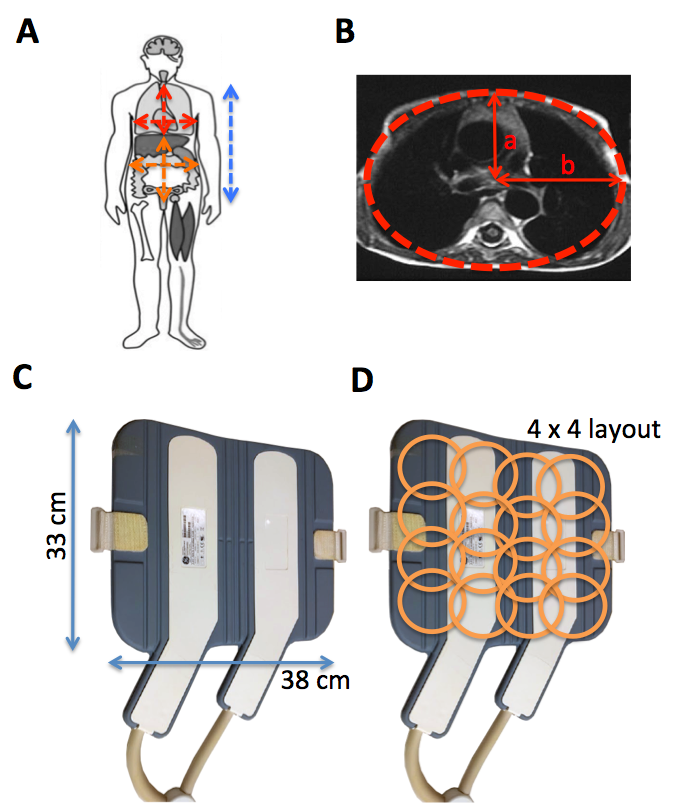
I. Patient Size: To characterize the size of pediatric patients, one month of pediatric abdominal and chest scans at a children’s hospital were measured - 87 scans comprised of 65 abdomen and 23 chest studies. Since the length of the torso was limited by the FOV of the scanner, 33 chest/abdomen/pelvis CT scans were included to accurately characterize patient torso length – Fig 2 A. To determine how much coverage an ideal array would need to provide, the half circumference of a patient was calculated using an elliptical fit – Fig 2 B.
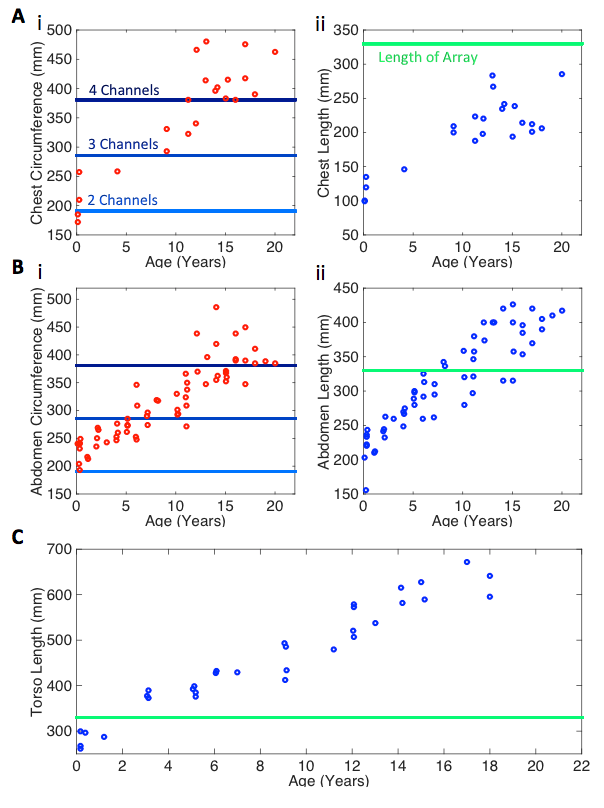
II. Current Array Size: The array currently used in our institution to scan pediatric patients was a 16 element (4x4) minimally flexible cardiac array – Fig 2 C and D. The dimensions of the array were overlaid onto the patient data to highlight current array fit– Fig 3. From here, we could see which age groups were using the entire array, 3/4 of the array, or half of the elements in the array. Note the gap between the 4-channel line and all patients age 0-5 suggesting that a 4th channel does not usually contribute any useful signal on these patients.
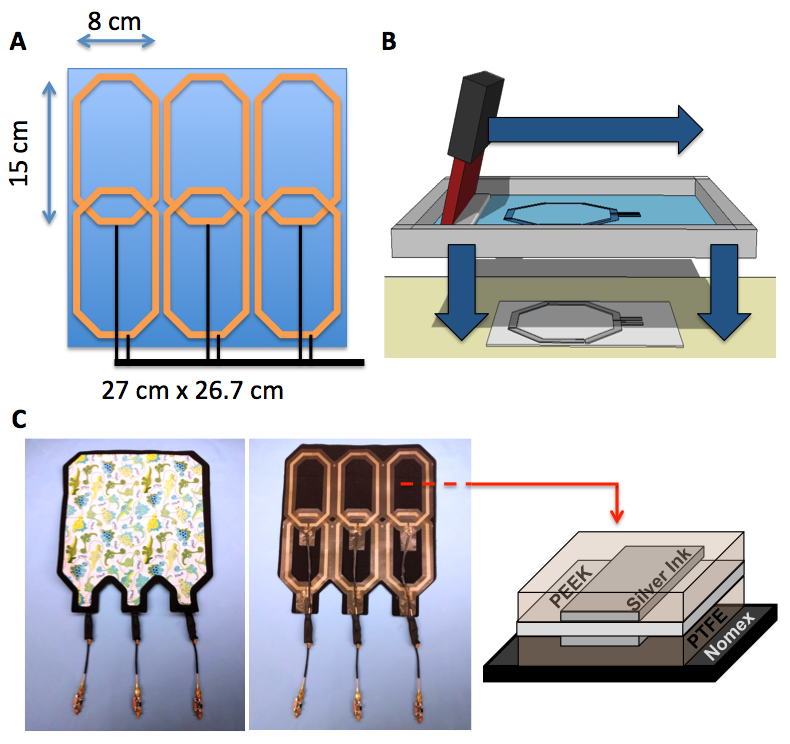
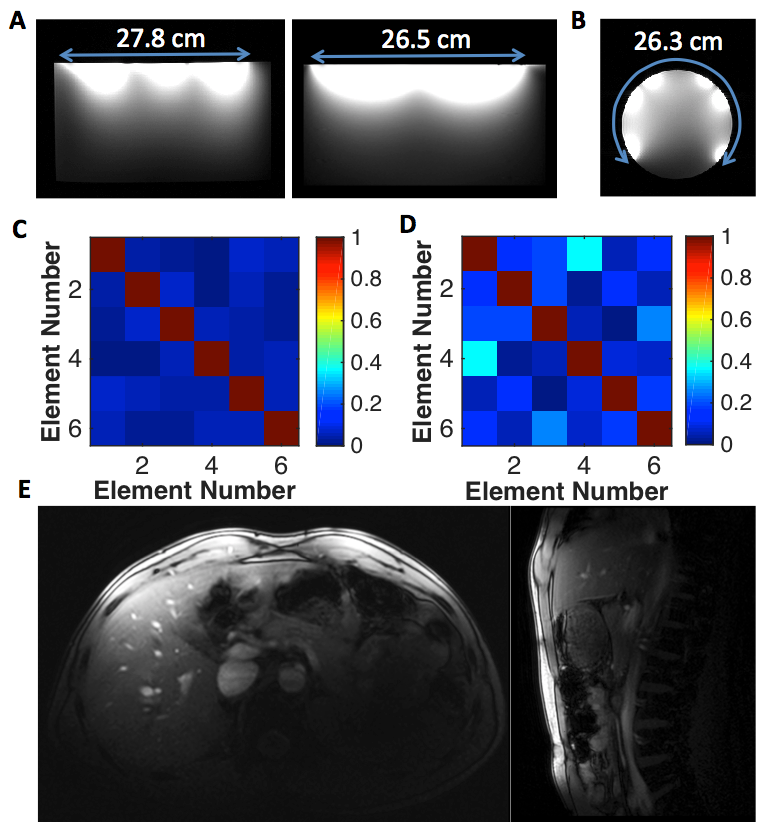
III. Size Optimize Array: Based on the patient data analysis, we determined that a 27 cm x 26.7 cm array would fit the torso of 0-2 year olds, and would cover the chest/abdomen of 3-5 year olds – Fig 4 A. To maintain low weight and reduce the complexity, we currently limit the number of elements in the array to 3 elements in the left-right direction and 2 elements in the superior-inferior direction. Therefore, each element would be 15 x 8 cm for a total of 6 elements in the anterior part of the array - Fig 4 A. Coils are overlapped lengthwise, but not across the body, contributing to coupling between the loops [6]. To demonstrate proof-of-concept, a 6-channel lightweight and flexible anterior portion of the array was built using screen printing. In screen printing, conductive traces 15 μm thick are deposited from solution onto 76 μm thick plastic substrates – Fig 4 B. The entire array is encapsulated in 76 μm of polytetrafluoroethylene then affixed onto a 200 μm thick fireproof fabric. Several phantoms and a volunteer were used to characterize the array. Fig 5A shows the array providing 27.8 cm x 26.5 cm of coverage on a phantom while Fig. 5B shows the array providing 26.3 cm of coverage wrapped around a cylinder. The coverage area is within 0.8 cm of the design goals detailed in Fig. 4. The noise correlation measurements shown in Fig 5 C and D show that there is some coupling between channels due to the under-lapped coil design but it is below 10% while the array is flat. As the array is flexed, the maximum correlation increases to 36%. Fig 5 E shows axial and sagittal cross-sections on an adult volunteer that have good coverage despite being intended for a pediatric patient. The array, including cabling, weighed only 341 g.
Conclusions and Outlook
Using patient data, knowledge of pediatric scan workflow, and alternate fabrication techniques, an extremely lightweight and flexible array for pediatric patients was constructed. The array produced high quality images on both phantoms and volunteers.Acknowledgements
We would like to thank Stanford’s Lucile Packard’s Children’s hospital for providing access to pediatric chest and abdominal images. Additionally, we thank Anita Flynn, Thomas Grafendorfer, James Tropp, Victor Taracila, and Fraser Robb, along with GE Healthcare, for guidance with electrical testing of coils.References
[1] S. Vasanawala, T. Grafendorfer, P. Calderon, G. Scott, M. Alley, M. Lustig, et al., "Millimeter Isotropic Resolution Volumetric Pediatric Abdominal MRI with a Dedicated 32 Channel Phased Array Coil," presented at the International Socieity of Magentic Resosnance and Medicine 19, Montreal, Canada, 2011.
[2] B. Keil, V. Alagappan, A. Mareyam, J. A. McNab, K. Fujimoto, V. Tountcheva, et al., "Size-optimized 32-channel brain arrays for 3 T pediatric imaging," Magn Reson Med, vol. 66, pp. 1777-87, Dec 2011.
[3] J. R. Corea, P. B. Lechene, M. Lustig, and A. C. Arias, "Materials and Methods for Higher Performance Screen-Printed Flexible MRI Receive Coils," Magn Reson Med, Sep 9 2016.
[4] J. R. Corea, A. M. Flynn, B. Lechene, G. Scott, G. D. Reed, P. J. Shin, et al., "Screen-printed flexible MRI receive coils," Nat Commun, vol. 7, p. 10839, 2016.
[5] B. Keil and L. L. Wald, "Massively parallel MRI detector arrays," J Magn Reson, vol. 229, pp. 75-89, Apr 2013.
[6] P. B. Roemer, W. A. Edelstein, C. E. Hayes, S. P. Souza, and O. M. Mueller, "The NMR phased array," Magn Reson Med, vol. 16, pp. 192-225, 1990.
Figures