4267
Investigating the compensatory mechanisms of the ageing brain in response to a sub-maximal exercise task1Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham, United Kingdom, 2MRC/ARUK Centre for Musculoskeletal Ageing Research, University of Nottingham, Nottingham, United Kingdom
Synopsis
Age-related alterations in cerebral vascular function may be better understood by investigating cerebral response to exercise. We performed a MR study involving low/moderate intensity exercise in healthy young and older subjects. We assess the effect of exercise on CBF response, cerebral oxygenation, and CMRO2. We also investigate the relationship of GM-volume and physical fitness with ageing. At rest, there was no difference between CBF and CMRO2 but an increase in oxygen extraction with age. On exercise the age-related increase in OEF remained, however CBF and CMRO2 were blunted in older subjects. GM-volume was found to be associated with VO2max.
Purpose
Understanding the mechanisms of cerebral response to acute exercise in the elderly may aid identification of age-related alterations in cerebral vascular function, particularly given associations between physical activity and mental health with age. Previous studies examining the impact of age on cerebral perfusion during exercise using transcranial Doppler (TCD) techniques have shown a significant blunting in cardiac output and cerebral artery blood velocity in older vs. younger people during exercise1,2. This was accompanied by an increase in cerebral metabolic rate of oxygen (CMRO2) on exercise which was similar for both older and younger participants, suggesting the age-related reduction in cerebral perfusion during exercise can be compensated for by greater brain oxygen extraction.
Aim
In healthy young and older volunteers, we used T2-Relaxation-Under-Spin-Tagging (TRUST)3,4 to assess measures of cerebral venous oxygenation (Yv) and oxygen extraction fraction (OEF) and, together with cerebral blood flow (CBF) and grey matter (GM) volume, we determine the CMRO2 at rest, in response to low/moderate intensity steady-state exercise and during recovery.Method
14 healthy male subjects were recruited to younger (N=6,21-26years,BMI 23.1±1.7(mean±SEM)) and older (N=8,58-70years,BMI 25.1±1.5) groups.
VO2max: Subjects underwent continuous, incremental supine exercise to determine maximal oxygen consumption (VO2max) using a MR compatible cycle ergometer (Lode) and on-line gas analysis (Cosmed).
Exercise task: MR data was acquired at rest, during 10min of steady-state exercise inside the scanner at workloads equivalent to 30% and 50% supine VO2max, and subsequent recovery.
MR acquisition: Data was acquired on a Philips 3T Achieva MR scanner (32-channel receive coil). 2D PC-MRA data was acquired to locate the superior sagittal sinus (SSS), L/R internal carotid arteries (ICA) and basilar artery (BA). At baseline, each workload and recovery period, Yv was acquired in the SSS using a TRUST MRI sequence (3.44x3.44x5mm3 voxels, inversion time 1022ms, four eTEs=1,40,80,160ms, labelling thickness 100mm/gap 22.5mm, TR=3000ms per label/control). Blood flow (velocity,flux) in L/R ICA and BA was measured using VCG-gated PC-MRI (TE/TR=6.5/15ms,FA=25°, FOV=280x77mm2,0.75x0.75x6mm3,SENSE4, vENC=100cm/s, NSA=2). Following the exercise protocol, an MPRAGE image (1mm3) was acquired to estimate GM-volume. In addition, 13 subjects were recruited to collect additional measures of VO2max and GM-volume.
Data analysis: MPRAGE data were segmented and GM-volume computed (normalized for subject head size) using SIENAX (FSL). TRUST data were processed following methods in Lu H et al.3, with SSS signal formed from (label-control) images, and the calculated T2 relaxation converted into Yv using a calibration plot5. OEF was calculated as the difference between arterial oxygenation (Ya) and Yv. GM-corrected CMRO2 (gmCMRO2) was quantified as described by Peng et al.4 accounting for age and sex. PC-MRI data were analysed using Q-Flow (Philips) for vessel area, velocity and flux in the L/R ICA and BA. Flux measures were summed to estimate ‘Total CBF’ and corrected for GM-volume (gmCBF).
Results
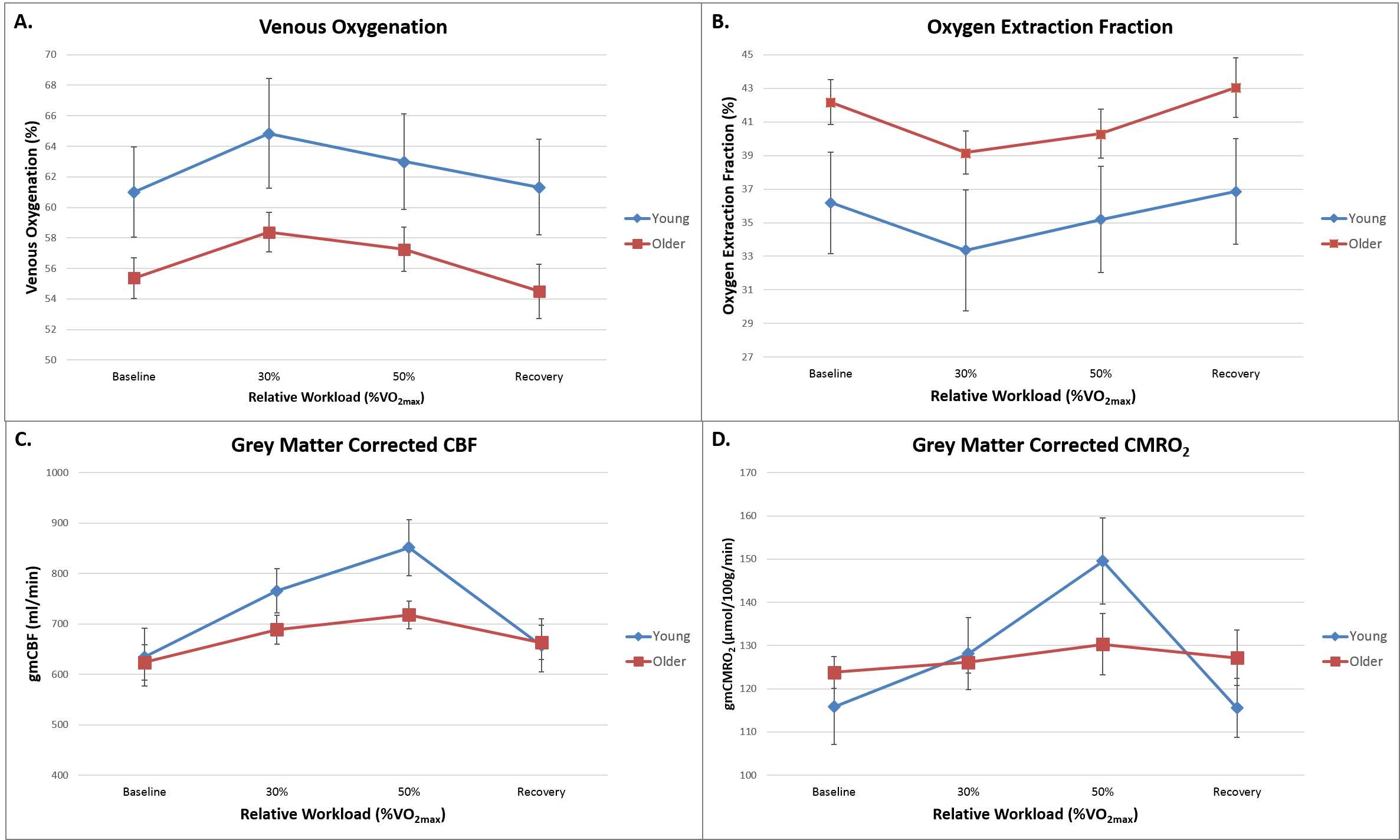
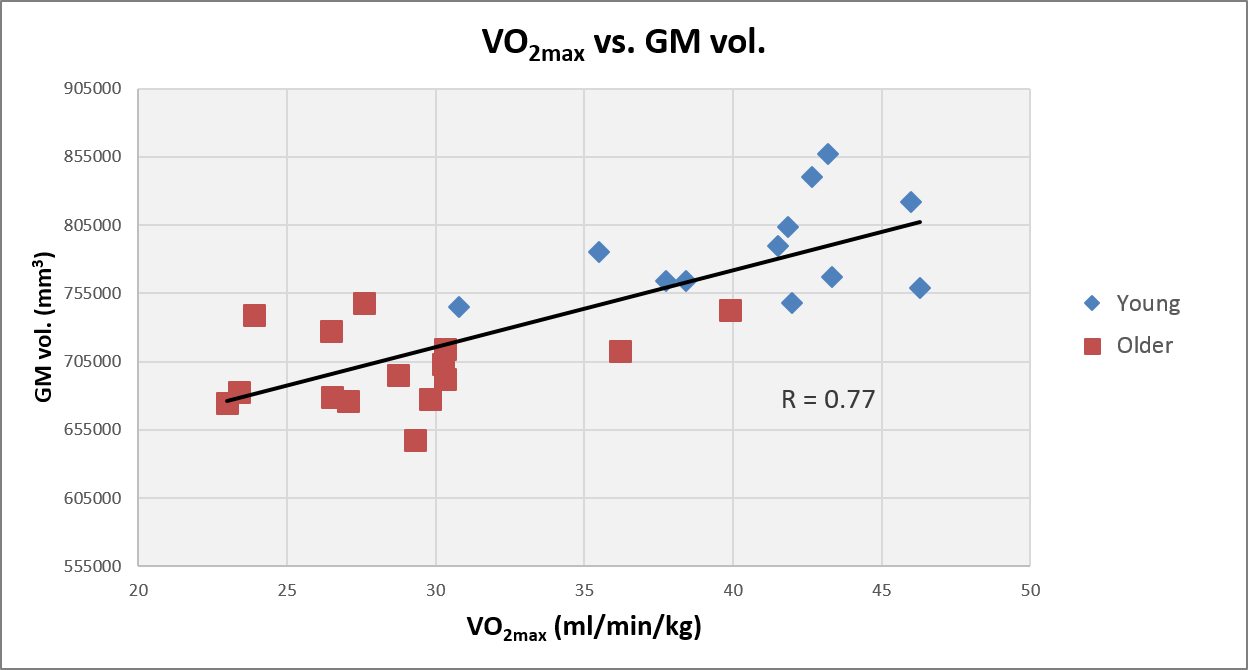
Supine VO2max was lower in older vs. younger subjects (30.8±5.0 vs. 43.6±1.8ml/min/kg) as was absolute maximum exercise workload (145±18 vs. 177±24W). Fig.1A shows Yv at rest, on exercise and during recovery for younger and older subjects. Fig.1B shows the corresponding OEF, indicating a greater OEF in older compared to young subjects across the exercise task (overall age effect p=0.0018, significant at rest and recovery (p<0.05)). Fig.1C shows a significant blunting of gmCBF in older subjects at 50% VO2max. Fig.1D shows gmCMRO2 change over the exercise task for both groups. Fig.2 shows a positive correlation between GM-volume and each individual’s VO2max (Pearson R =0.776, p<0.001).Discussion
At rest there was no significant difference in gmCBF and gmCMRO2 between young and old, however oxygen extraction was significantly greater in older subjects (p=0.035), suggesting decreased metabolic efficiency with age. On exercise (combined 30/50% VO2max), an age-related increase in OEF remains (p=0.044). Blunting of gmCBF in older subjects compared to young at 50% VO2max suggests the muscle steal of cardiac output is sufficiently large to limit brain perfusion in older people. Further, a trend for blunting of CMRO2 in older compared to younger subjects at 50% VO2max, suggests that greater OEF does not fully compensate for lower CBF at this workload in the older group. However, this requires a larger group size for confirmation. We also show that, across a wide age range of subjects, GM-volume is associated with an individual’s VO2max, suggesting a functional relationship between GM-volume and cardio-respiratory fitness and health.Conclusion
In agreement with TCD, we show a reduction in gmCBF and a greater OEF during sub-maximal, steady-state exercise in older vs. younger volunteers, warranting further investigation at higher workloads. The association between VO2max and GM-volume suggests that maintaining physical activity and cardio-respiratory fitness may have a brain protective effect.Acknowledgements
We thank Hanzhang Lu for sharing TRUST methodology. Andrew Hale holds a MRC-ARUK Centre for Musculoskeletal Ageing Research studentship.References
[1] Fisher et al. J Physiol. 591(7):1859-70, 2013. [2] Braz ID, Fisher JP. J Physiol. 594(16):4471-83, 2016. [3] Lu H, Ge Y. Magn Reson Med. 60(2):357–63, 2008 [4] Peng SL et al. Neuroimage. 98:176-183, 2014. [5] Zhao JM et al. Magn Reson Med. 58:592-597, 2007.Figures