4207
Image Quality Comparison of High Resolution PC-MRA (4D-Flow) with Time of Flight in Healthy Volunteers1Department of Radiological Sciences, University of California, Los Angeles, CA, United States
Synopsis
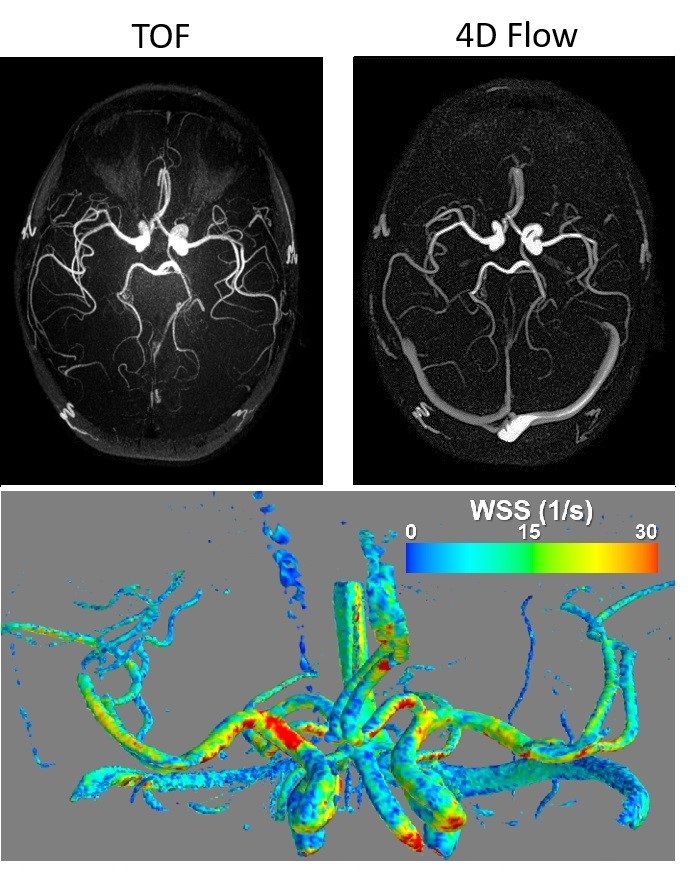
In this study, image quality of high resolution PC-MRA (4D Flow) and 3D-TOF was compared. Ten healthy volunteers were scanned with high resolution 4D-Flow and 3D-TOF angiograms at 0.5 mm isotropic spatial resolution in clinically-useful scan times of 7 and 12 minutes. There was no significant difference in image quality between 4D Flow and 3D-TOF in both source images and MIPs. 4D Flow acquisitions were velocity encoded, allowing hemodynamic evaluation of intracranial structures. This study demonstrated that phase-contrast techniques such as 4D-Flow have comparable image quality to 3D-TOF while obtaining velocity measurements, showing promise as a viable alternative to 3D-TOF.
Purpose
3D-TOF has long been used for the evaluation of intracranial stenoses, aneurysms, and AVMs, allowing high resolution images to be obtained without intravenous contrast with relatively short scan time. PC-MRA techniques are velocity encoded, allowing for hemodynamic evaluation, however they are less frequently used clinically because of long scan times and lower spatial resolution. With novel accelerated radial 4D PC-MRA techniques such as PC-VIPR and PC-SOS [1-3], higher resolution images can be obtained in clinically-useful scan times. A single non-contrast examination providing high-quality angiography and hemodynamic evaluation is clinically useful for the assessment of intracranial lesions. We compare the image quality of 4D Flow PC-MRA, at 0.5 mm isotropic spatial resolution with 3D-TOF in ten healthy volunteers.Materials & Methods
10 healthy volunteers were scanned using a Siemens Prisma 3.0T MRI scanner. Source/MIP images were obtained using 4D-Flow and 3D-TOF sequences. TOF parameters:FOV=220x165x52 mm, spatial resolution=0.5mm, flip=20o, grappa=4, slabs=4, scan time=7:00. 4D-Flow:(modified stack of stars technique[3]),25,000 projections/velocity encode, Venc=80 cm/s, scan time=12:00, resolution=0.50 mm, TE/TR=4.1/8.1 ms, flip angle=8o FOV=220x220x52 mm. Two experienced readers scored image quality in the ICA, basilar, ophthalmic, anterior choroidal, P1-3, A1-3, and M1-3 arterial segments, following the protocol used in our previous image quality study[4]. Images were scored using a 4-point Likert scale(1=poor visualization; 2=visualized but not of diagnostic quality; 3=good visualization of diagnostic quality; 4=excellent diagnostic quality). A Mann-Whitney U-test was performed to compare mean image quality for all vessels, major first-order branches (ICA, M1, P1, A1) and second and third order branches (A2, A3, P2, P3, M2, M3, ophthalmic, and anterior choroidal arteries) for both source images and MIPs.Results
Both techniques had excellent visualization of all major vessels on both source images and MIPs (image quality 4.0±0).For source images there was no significant difference between 4D Flow and 3D-TOF for all vessels (3.84±0.49 TOF, 3.81±0.55 4D-Flow, p=0.87) or 2nd/3rd order branches (3.74±0.60 TOF, 3.71±0.67 4D-Flow, p=0.82). For MIPs there was also no significant difference between image quality between 4D Flow and 3D-TOF for all vessels (3.75±0.70 TOF, 3.64±0.88 4D Flow, p=0.51) or for 2nd/3rd order branches (3.60±0.85 TOF, 3.43±1.05 4D Flow, p=0.37). Both observers commented that the 3D-TOF images were grainy in the region of the cavernous sinus and supraclinoid ICA; this was not observed on the 4D Flow images, which subjectively were sharper for the assessment of the major arterial branches and 2nd/3rd order ACA/PCA/MCA branches. The 4D Flow images were also significantly better on the source images when compared to the MIPs. Both observers also noted that susceptibility artifact in the optic nerve canal degraded image quality of the ophthalmic arteries on the 4D-Flow images, resulting in lower grading for that vessel; the remainder of those vessels demonstrated excellent image quality.Discussion
PC-MRA techniques have been an active area of investigation for evaluation of intracranial pathology because their velocity encoding allows for assessment of hemodynamics. The limitations of the technique have traditionally been long scan times and insufficient spatial resolution. The advent of radial techniques such as PC-VIPR [1,4] have allowed for relatively high resolution (0.7 mm isotropic) whole-brain acquisitions to be performed in approximately 5 minutes, with acceptable image quality. In a previous study [4]; we found PC-VIPR to have higher image quality than 3D-TOF and no significant difference in image quality when compared to digital subtraction angiography (DSA) in the evaluation of AVMs. This protocol is well-suited for the evaluation of arteriovenous malformations and hemodynamic differences in stable and unstable AVM patients were noted in a previous study.[5] However, for the evaluation of smaller intracranial lesions such as aneurysms, which may be as small as 3-4 mm, higher spatial resolution is needed in order to properly assess hemodynamics. PC-SOS is a technique allowing high in-plane spatial resolution (0.4x0.4x1.0 mm) which is useful for hemodynamic assessment; however, an isotropic technique allows greater clinical flexibility. In this study, we demonstrated the capabilities of 4D-Flow, a radial technique which has an isotropic spatial resolution of 0.5 mm(identical to 3D-TOF) and showed no significant difference in image quality when compared to 3D-TOF in both major intracranial vessels and 2nd/3rd order branches, while simultaneously acquiring velocity information which was used to calculate hemodynamic data such as flow and WSS. In the future, 4D-Flow techniques may represent viable alternatives to 3D-TOF that also acquire hemodynamic data.Conclusion
Conclusion: 4D Flow is a high-resolution phase-contrast technique with 0.5 mm isotropic spatial resolution that demonstrated no significant difference in image quality when compared to 3D-TOF in both major vessels and 2nd/3rd order branches.Acknowledgements
Funding support from the UCLA Department of Radiological Sciences.References
1. Chang, W, Huang, M, and Chien, A.Emerging techniques for the non-invasive imaging of intracranial vascular pathology, a review. Neuroradiol J. 2015 Feb;28(1):19-27.
2. Johnson, K., Lum, D., Turski, P., et al. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. Magn Reson Med. 2008 Dec;60(6):1329-36.
3. Kecskemeti, S., Johnson, K., Wu, Y., et al. High Resolution 3D Cine Phase Contrast MRI of Small Intracranial Aneurysms using a Stack of Stars k-Space Trajectory J Magn Reson Imaging. 2012 Mar; 35(3): 518–527.
4. Chang, W., Loecher, M, Johnson, K. et al. Fast Contrast Enhanced 4D MRA and 4D Flow MRI using Constrained Reconstruction (HYPRFlow): Potential Applications for Brain Arteriovenous Malformations, AJNR Am J Neuroradiol. 2015 Jun;36(6):1049-55
5. Chang, W., Loecher, M., Wu, Y., et al. Hemodynamic Changes in Patients With Arteriovenous Malformations Assessed Using High Resolution 3D-Radial Phase Contrast Magnetic Resonance Angiography, AJNR Am J Neuroradiol 2012 33: 1565-1572
Figures