4201
Navigating the Brachial Plexus: An MRI Visual Primer1Radiology, Santa Barbara Cottage Hospital, Santa Barbara, CA, United States
Synopsis
This educational exhibit provides an up-to-date, practical approach for MRI evaluation of the brachial plexus.
Purpose
The inherent complexity of the brachial plexus has the potential to make magnetic resonance imaging (MRI) evaluation a daunting task. In response to these challenges, this educational exhibit aims to make the anatomy, MRI techniques, and pathology easily approachable with the end goal of empowering trainees and general radiologists to approach these exams with confidence.Outline of Content
While exams can be performed on a 1.5 Tesla (T) or 3T scanner, images are ideally obtained on a 3T MRI and a practical approach for developing MRI protocols for clinically relevant and efficient image acquisition is discussed. Schematic and MRI anatomy is correlated for the benefit of the viewer, with attention to vital landmarks and sites of potential pathology. An essential part of interpretation includes pre- and post-ganglionic localization, segmental location (i.e. within the roots, trunks, etc…), as well as the anatomic relationship with surrounding structures. Building upon the anatomy, a workable method for detecting and organizing brachial plexus pathology is presented. Evaluation includes a strict search pattern that utilizes three planes for optimal assessment of specific areas of interest and takes in account lesion morphology and pattern of enhancement to help confirm the location. Traumatic and non-traumatic pathologies will be discussed with a focus on common etiologies, although more unusual disease processes, including herpes zoster and heroin-related brachial plexopathy cases will also be presented. As clinical history plays an important role in synthesizing an appropriate differential for brachial plexus pathology, a case-based approach will be utilized for presentation and educational purposes.Summary
MRI evaluation of the brachial plexus can be confidently and efficiently interpreted with a fundamental understanding of MRI protocols, brachial plexus anatomy, and pathology.Acknowledgements
No acknowledgement found.References
Castillo M. Imaging the Anatomy of the Brachial Plexus: Review and Self-Assessment Module. AJR 2005; 185:S196-204
Vijayasarthi A, Chokshi F. MRI of the brachial plexus: A practical review. Applied Radiology 2016; May:9-18
Yoshikawa T, Hayashi N. Brachial Plexus Injury: Clinical Manifestations, Conventional Imaging Findings, and the Latest Imaging Techniques. RadioGraphics 2006; 26:S133–S143
Figures

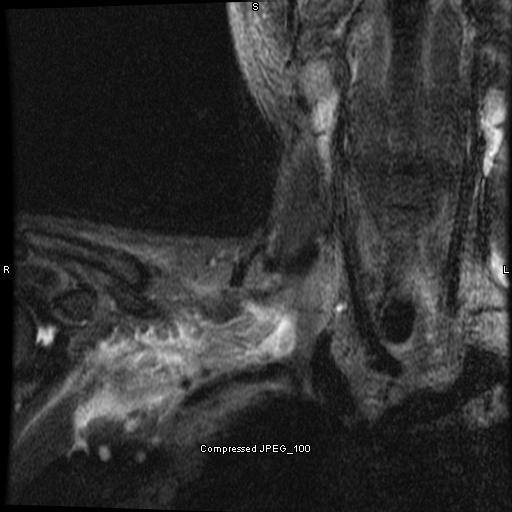
Heroin Plexopathy.
Coronal T2 fat-saturated image demonstrates enlargement and hyperintense signal in the right brachial plexus in a patient with a history of intravenous heroin abuse who presented to the emergency department with pain and weakness in the right upper extremity.

Heroin Plexopathy.
Coronal T1 fat-saturated and gadolinium enhanced image demonstrates mild enhancement of the right brachial plexus in a patient with a history of intravenous heroin abuse who presented to the emergency department with pain and weakness in the right upper extremity.
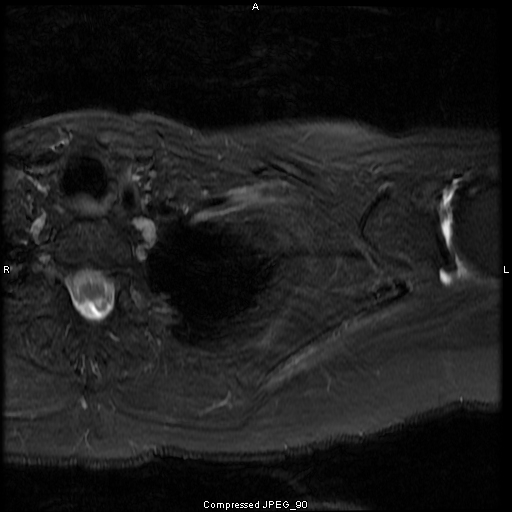
Herpes Zoster Plexopathy.
Axial T2 fat-saturated image demonstrates enlargement and hyperintense signal in the left brachial plexus in a patient with herpes zoster who presented with left upper extremity weakness.
Brachial Plexus Traction Injury.
Coronal T2 fat-saturated image demonstrates hyperintense signal in and surrounding the right brachial plexus in a patient who had persistent right upper extremity weakness following trauma.