4186
Active and passive fMRI for preoperative localization of motor function areas in brain tumor patientsChen Niu1, Xiao Ling1, Pan Lin2, Kun Zhang3, Xin Liu4, Liping Guo1, Wenfei Li1, Hao Song2, Ming Zhang1, and Maode Wang5
1Department of Medical Imaging, The First Affiliated Hospital of Xi'An Jiaotong University, Xi'An, People's Republic of China, 2Key Laboratory of Biomedical Information Engineering of Education Ministry, Institute of Biomedical Engineering, Xi’an Jiaotong University, 3Department of Electronics Engineering, Northwestern Polytechnical University, 4Technical University Munich, 5Department of neurosurgery, The First Affiliated Hospital of Xi'An Jiaotong University, Xi'An, People's Republic of China
Synopsis
The aim of this study is to investigate whether there is consistency between active and passive movement in patients with brain tumors. Two motor tasks (active and passive hand movement) were applied to brain tumor patients. Our results demonstrate that there is no statistical difference of activation intensity between active hand movement and passive hand movement in patients with brain tumors. Our results suggest that passive movement fMRI provides a potential method for presurgical mapping in cases where patients are unable to comply with task instructions.
Introduction:
Task-based functional MRI is a non-invasive technique that can be used in neuronavigational planning, allowing the surgeon to achieve maximal resection while minimizing the risk of neurological impairments.1 However, many patients with brain tumors are excluded from functional motor mapping due to their inability to perform relevant task. Previous studies showed that passive movement was able to produce activation of most of the cortical areas traditionally described in motor system in some brain diseases. 2, 3 The aim of this study is to investigate whether there is consistency between active and passive movement in patients with brain tumors.Materials and Methods:
Twenty patients with brain tumors (right-handed, 9 males and 11 females, age ranged from 17-81 years, mean age 49.7±17.5 years) were enrolled in this study. We employed a 3.0-T GE scanner equipped with an eight-channel head coil. Both structural images (3D FSPGR 1x1x1 mm3, 140 slices) and BOLD EPI data (TR/TE = 2500/40 ms, flip angle=90°, 3.75x3.75x3mm3) were acquired. Two motor tasks (active and passive hand movement) were applied to all patients. The experiments were arranged in block designs, consisting of five blocks of movement task and six blocks of rest period, each block lasts for 30 seconds. During the active hand movement task, patients were asked to repetitively open and close the hand at a steady frequency. The commands were presented by an LCD projector and viewed on a mirror placed above the patient’s head. They were asked to simply lie still during the rest period. During the passive hand movement task, patients were asked to relax while examiner repetitively opened and closed patient’s one hand at the same frequency as in the active movement task. During the rest period, the examiner kept holding the patient’s hand and they were asked to lie still. The task fMRI data was analyzed with FSL software. The first 4 scans were discarded to allow for initial signal stabilization and then motion correction was conducted using FLIRT. Spatial smoothing was performed with a 6-mm FWHM Gaussian kernel. The functional images were normalized to the MNI152 standard brain space. General linear model (GLM) analysis was carried out using FSL FEAT. Higher-level analysis was carried out using FLAME. Z statistic images were thresholded using clusters determined by Z >2.3, a corrected cluster significance threshold of p<0.05. The key motor regions included left primary motor cortex (LPMC), right primary motor cortex (RPMC) and supplementary motor area (SMA) based on motor task functional mapping. We further performed the two-sample t tests on PMC and SMA activation intensity between active and passive movement to evaluate the activation differences of motor cortex in patients with brain tumors.Results:
A comparison of activation mapping between unilateral left hand passive movement and active hand movement is shown in Figure 1a, and a comparison of activation mapping between unilateral right hand passive movement and active hand movement is shown in Figure 1b. The overlapping of activations maps indicate that there is consistency between active hand movement and passive hand movement. Furthermore, we compared the activation intensity of passive and active motion in PMC and SMA, the results showed no significant difference between them (P > 0.05), as illustrated in Fig.2.Discussion and Conclusions:
Our results demonstrated that there is no statistical difference of activation intensity between active hand movement and passive hand movement in patients with brain tumors. This might be because the somatosensory stimulation of passive hand movement, including tactile and proprioceptive input, could activate brain sensorimotor network, indicating a tight connection between sensory and motor cortical activation.4 In summary, our results suggest that passive movement fMRI provides a potential method for presurgical mapping in cases that patients are unable to comply with task instructions. This approach could assist in assessing the risk of a surgery, enhancing surgical performance and preserve brain function.Acknowledgements
This work was supported by the National Natural Science Foundation of China (61401363, 61262034), by the Fundamental Research Funds for the Central Universities of China (1191320118).References
1. Hervey-Jumper SL, Berger MS. Maximizing safe resection of low- and high-grade glioma. J Neurooncol. 2016 Nov;130(2):269-282.
2. Fu Y, Zhang Q, Zhang J, et al. Comparative Functional MRI Study to Assess Brain Activation Upon Active and Passive Finger Movements in Patients with Cerebral Infarction. Eur Neurol 2015;73(1-2):13-19.
3. Dinomais M, Chinier E, Lignon G, et al. The effect of video-guidance on passive movement in patients with cerebral palsy: fMRI study. Res Dev Disabil. 2013, 34(10): 3487-3496.
4. Kato H, Izumiyama M. Activation of Brain Sensorimotor Network by Somatosensory Input in Patients with Hemiparetic Stroke: A Functional MRI Study. INTECH Open Access Publisher, 2013.
Figures
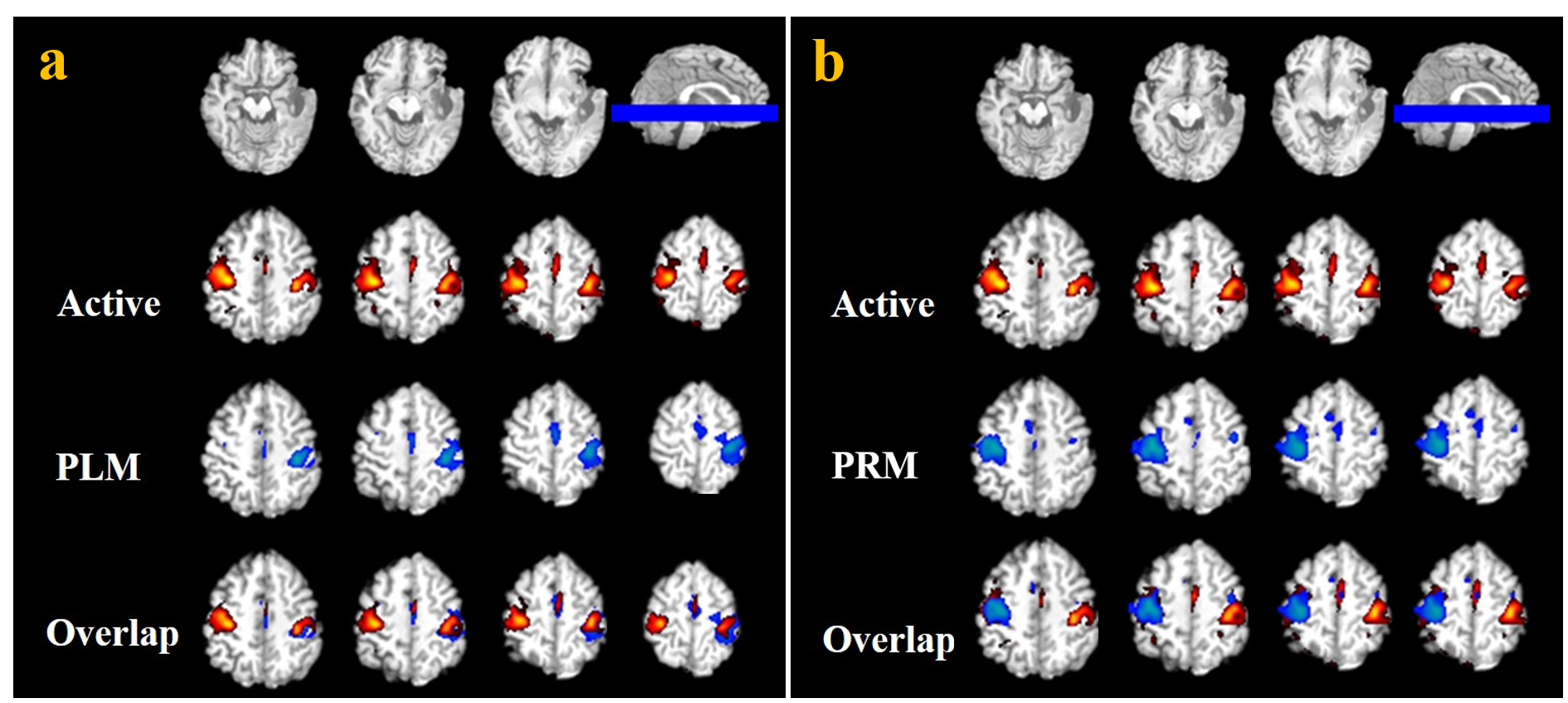
Fig.1 A comparison of activation maps between active hand movement and a) unilateral left hand passive movement; b) unilateral right hand passive movement. Structure images, activation maps of bilateral hands active movement, passive left-hand movement (PLM) and passive right-hand movement (PRM), and the overlapping of activations maps are shown from top to bottom on (a) and (b) respectively.
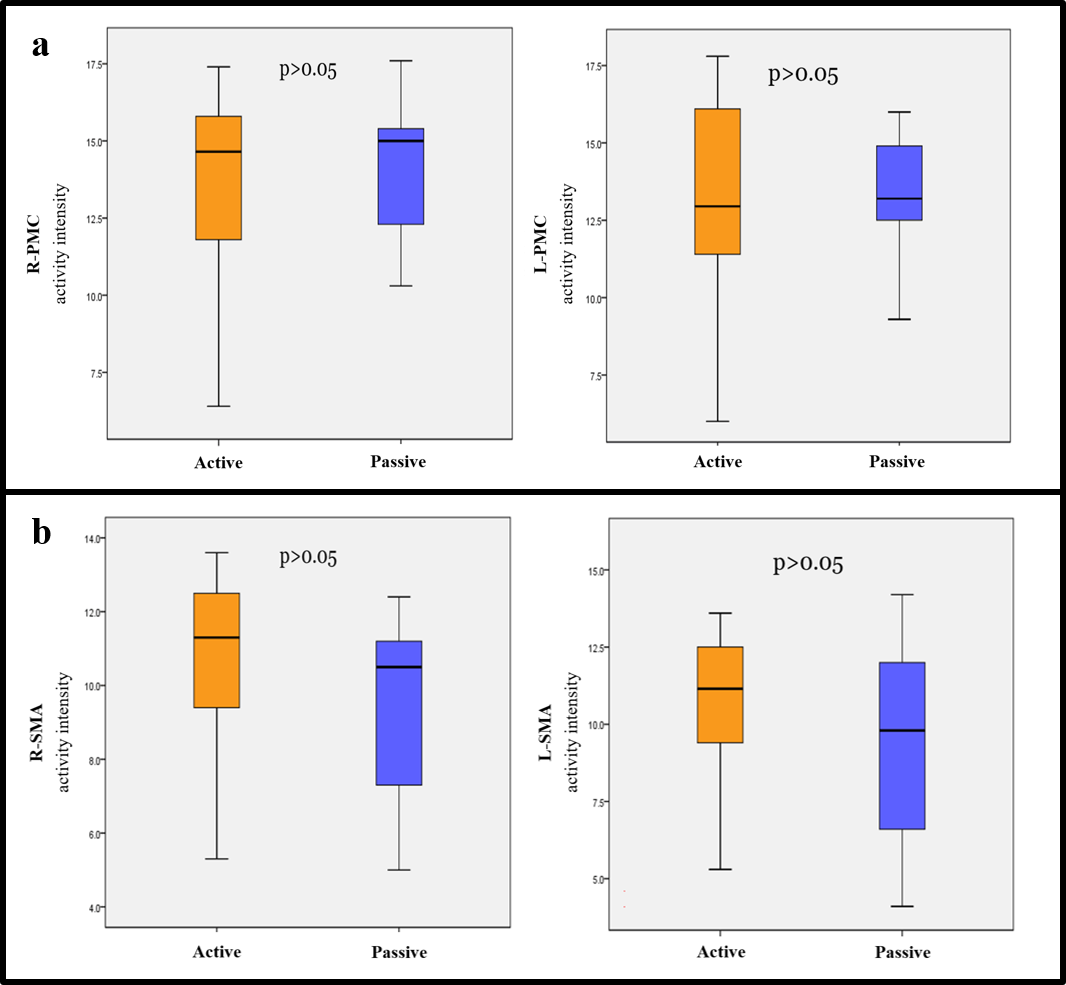
Fig.2. Comparison
of activation intensity in the PMC (a) and SMA (b) after with active and
passive movement in patients with brain tumors.