4181
Non-invasive, contrast-exempt (NICE) assessment of glioblastoma (GBM) using multi-slice ASL and iVASO imaging1Radiology, University of Washington, Seattle, WA, United States, 2University of Washington
Synopsis
Assessment of cerebral and tumor perfusion has frequently been advocated for initial prognostication, and evaluation for possible progression, of primary brain tumors, historically accomplished via intravenous injection of a gadolinium-based contrast agent (GBCA). The potential for intracranial and corporeal deposition of GBCA invites the development and optimization of non-invasive, contrast-exempt (NICE) methods to assess cerebral perfusion. We sought to develop and implement NICE spin-label-based methods incorporating cerebral blood flow (CBF) and volume (CBV) assessment, applied in treated GBM patients.
INTRODUCTION
Assessment of
cerebral and tumor perfusion has frequently been advocated for initial
prognostication, and evaluation for possible progression, of primary brain
tumors, historically accomplished via intravenous injection of a
gadolinium-based contrast agent (GBCA)1. The potential for intracranial and corporeal deposition of GBCA2 invites
the development and optimization of non-invasive, contrast-exempt (NICE)
methods to assess cerebral perfusion. While arterial spin
labeling (ASL) is now a clinically
established method to assess perfusion, inflow-vascular space occupancy (iVASO)
is still an experimental approach to evaluate CBV3, 4. Multiple
studies show that CBV values derived from iVASO correlate well with contrast
enhancement measures in neuronal disorders and have reproducibility similar to
that of ASL4-6. While ASL and
iVASO has been used separately for GBM evaluation in previous studies, a systematic
combined ASL and iVASO protocol to evaluate GBMs and treated GBMs has not yet
been performed7. Our goal was to perform preliminary validation of a
NICE protocol for CBF and CBV parametric map generation in patients with
treated GBM using ASL and iVASO and compare it with Gadolinium-based tumor
evaluation.
METHODS
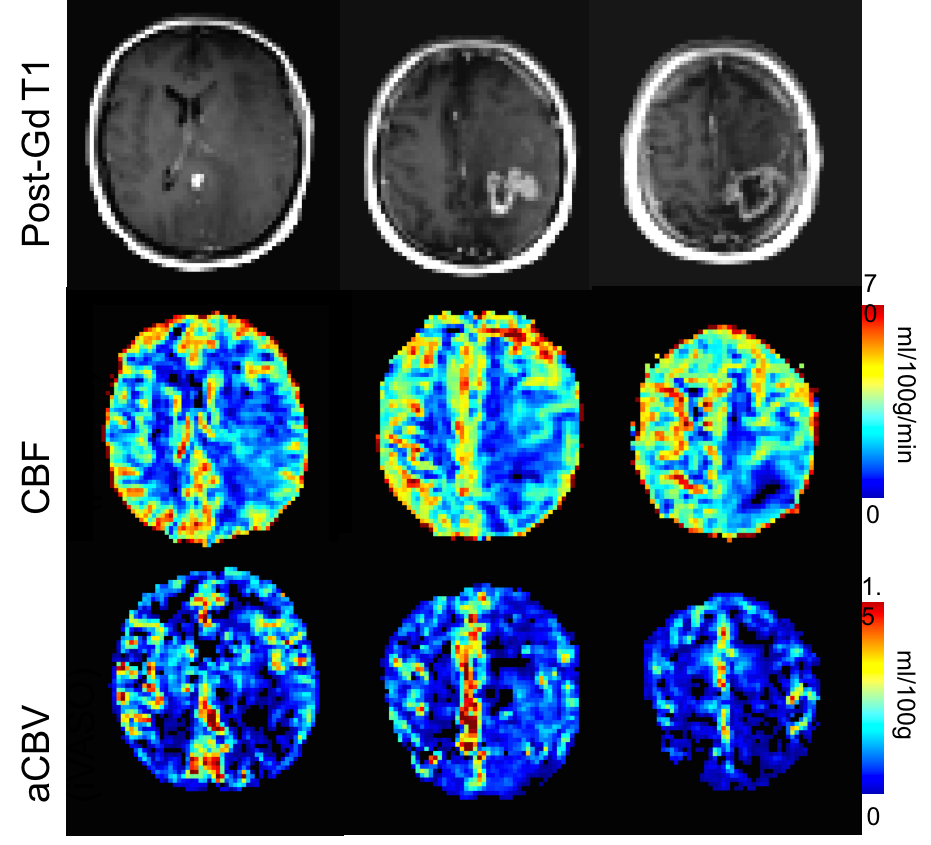
Initial work: We performed multi-slice iVASO using a 3D-GRASE readout in 10 healthy young adults and measured cortical arterial CBV to be 0.7±0.2 ml/100g. Note that iVASO measures pre-capillary vascular components in healthy tissue and hence is lower than the total CBV, often measured with Gadolinium-based CBV measurements. Experiment: Enlisted GBM patients underwent sequential 3D T1 (pre and post Gadolinium contrast injection), multi-slice iVASO (3D GRASE) acquisition, and pCASL acquisition using a 12-channel SENSE head-coil on a Philips 3T Achieva scanner. The pCASL parameters were: matrix = 96×96×20, spatial resolution = 3×3×5 mm3, flip angle = 90°, TE = 19 ms, TR = 5000 ms, label duration = 1800 ms, post-labeling delay = 2000ms, 30 control/null pairs and a M0 image with TR = 10000 ms, SENSE factor = 2.5. iVASO acquisitions were performed at TR of 5000 ms and TI of 1190 ms to capture the steady-state blood water signal nulled in null acquisitions even in the slow perfusion regions of the tumor, matrix = 96×96×12, spatial resolution = 3×23×5 mm3, flip angle = 90°, TE = 19 ms, 30 control/null pairs and a M0 image without iVASO preparation at TR = 10000 ms, R = 2.5. The multi-slice 3D GRASE imaging parameters were identical except TE = 22 ms and k-Space profile = low-high, turbo direction = Z, readout = 300 ms, SENSE factor = 2.5 (RL) and 2 (AP). Analysis: Both, iVASO and PCASL images were motion-corrected and registered to the respective M0 image. aCBV was calculated as outlined in previous studies4,5. CBF was calculated based on the ISMRM’s recommendations for quantification of pCASL data. Post-contrast T1 images were compared with CBF and aCBV maps to determine perfusion characteristics of GBM i.e. degree of perfusion and blood volume as a measure of angiogenesis.RESULTS
Four GBM subjects (age = 45.5±12.2 years;3F/1M) with varying degrees of therapy provided informed consent in this prospective, preliminary pilot study. Figure 1 depicts a large, peripherally enhancing tumor with central necrosis located in the right parietal lobe. Corresponding parametric NICE images demonstrate no compelling increase in CBF or CBV, suggesting a diagnosis of pseudoprogression rather than true progression, and commensurate with treatment effects from recent chemoradiation. The remaining three cases status post chemoradiation and surgery demonstrated expected minimal curvilinear enhancement about a resection cavity without significant compelling increased regional CBF and/or CBV to suggest tumor recurrence/progression.DISCUSSION
We demonstrate that a NICE protocol, allowing for contrast-free evaluation of tumor and cerebral perfusion can be appropriately applied in treated GBM patients. The derived CBF and CBV maps provide expected peritumoral and intratumoral results that may aid in modulating targeted tumor therapies. Moreover, tumoral angiogenesis, which is crucial for the survival and growth of GBM, is remarkably heterogeneous and differs significantly from normal vasculature with regard to structure, function, and organization8. In this small clinical sample, we identified one subject status post temozolomide chemoradiation (Fig. 1) with demonstrated antiangiogenic treatment effects (non-elevated regional CBF and CBV) and without definite evidence to suggest tumor progression despite residual, peripherally enhancing tumor, the latter suggesting leakage of GBCA beyond an injured BBB. Future studies will compare the proposed NICE CBF/CBV protocol for with the currently accepted GBCA-dependent methods of dynamic susceptibility contrast (DSC) perfusion-weighted imaging in a treated GBM patient population.CONCLUSION
Implementation of a NICE CBF/CBV protocol is feasible in a clinical population of treated GBM patients and may aid in modulating therapy in this population.Acknowledgements
No acknowledgement found.References
1. Essig M, Nguyen TB, Shiroishi MS, et al. Perfusion MRI: the five mostfrequently asked clinical questions. AJR Am J Roentgenol 2013;201:W495–510.
2. McDonald RJ, McDonald JS, Kallmes DF, et al. Intracranial Gadolinium Depositionafter Contrast-enhanced MR Imaging. Radiology. 2015 Jun;275(3):772-82.
3. Alsop DC, Detre JA, Golay X, Günther M, Hendrikse J, Hernandez-Garcia L, Lu H, MacIntosh BJ, Parkes LM, Smits M, Osch MJ. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magnetic resonance in medicine. 2015 Jan 1;73(1):102-16.
4. Donahue MJ, Sideso E, MacIntosh BJ, Kennedy J, Handa A, Jezzard P. Absolute arterial cerebral blood volume quantification using inflow vascular-space-occupancy with dynamic subtraction magnetic resonance imaging. Journal of Cerebral Blood Flow & Metabolism. 2010 Jul 1;30(7):1329-42.
5. Rane S, Talati P, Donahue MJ, Heckers S. Inflow-vascular space occupancy (iVASO) reproducibility in the hippocampus and cortex at different blood water nulling times. Magnetic resonance in medicine. 2015 Jul 1.
6. Huber L, Ivanov D, Guidi M, Turner R, Uludag K, Möller HE, Poser BA. Functional cerebral blood volume mapping with simultaneous multi-slice acquisition. NeuroImage. 2016 Jan 15;125:1159-68.
7. Donahue MJ, Blakeley JO, Zhou J, Pomper MG, Laterra J, van Zijl P. Evaluation of human brain tumor heterogeneity using multiple T1-based MRI signal weighting approaches. Magnetic resonance in medicine.2008 Feb 1;59(2):336-44.
8. Nagy JA, Chang SH, Shih SC, et al. Heterogeneity of the tumor vasculature. Sem Thromb Hemost. 2010;36(3):321–331.
Figures