4153
An animal model of comorbid cerebral hypoperfusion and metabolic syndrome1Cellular and Molecular Medicine, The University of Ottawa, Ottawa, ON, Canada, 2Medical Imaging, The Ottawa Hospital, Ottawa, ON, Canada, 3The Ottawa Hospital Research Institute, Ottawa, ON, Canada, 4Radiology, The University of Ottawa, Ottawa, ON, Canada, 5Cellular and Molecular Medicine, The University of Ottawa, 6Canadian Partnership for Stroke Recovery
Synopsis
Vascular cognitive impairment (VCI) arises from chronic cerebral hypoperfusion and is characterized by executive dysfunction, memory problems, and motor impairments. In countries where people eat highly processed, energy-dense food, there are high rates of VCI. Poor diet is also linked to metabolic syndrome, which is also associated with cognitive dysfunction. Metabolic syndrome and VCI commonly coexist within cardiovascular patients. Due to the translational failure of many promising preclinical treatments for cardiovascular disease, researchers are trying to incorporate human comorbidities within animal disease models. Here, we develop a rat model which combines cerebral hypoperfusion with an unhealthy diet.
Introduction
Vascular cognitive impairment (VCI) is a form of small vessel disease arising from chronic cerebral hypoperfusion, characterized by executive dysfunction, memory problems, and motor impairments. Westernized countries, where consumption of highly processed, energy-dense food is frequent, exhibit high rates of VCI. Such lifestyles are linked to metabolic syndrome (obesity, hyperglycemia, hypertension, dyslipidemia, hyperinsulinemia), which is also associated with cognitive dysfunction. Because of the shared cardiovascular nature of VCI and metabolic syndrome, these two conditions commonly coexist. VCI and metabolic syndrome are routinely associated with damage to the hippocampus and white matter, structures that are especially vulnerable to global ischemia (1-5).
Due to the translational failure of many promising preclinical treatments for cardiovascular disease, researchers are trying to incorporate human comorbidities within animal disease models, thereby ensuring a more realistic manifestation of the interplay between conditions (6-10). Here, we develop a rat model that combines cerebral hypoperfusion with a high fat, ultra-processed junk food diet (11-14). We hypothesized that this combination would exacerbate hippocampal and white matter pathology and worsen cognitive deficits.
Methods
N=101 rats were randomly assigned to 4 treatment groups. Half consumed a "cafeteria" (CAF) diet comprised of rotating combinations of 16 grocery store-purchased junk foods or standard (SD) rat chow (Fig 1). Within each diet group, rats underwent 2-vessel carotid artery occlusion (2VO) or sham.
Metabolic blood data were monitored (Fig 2). Subsets of rats were MRI'd at 1 week, 1 month, or 2 months post-surgery. Following MRI, some animals were sacrificed for histological analysis of hippocampal CA1 cell density. Other animals were MRI’d longitudinally and subjected to cognitive testing (object recognition and Morris Water Maze).
MRI perfusion measurements were performed using a 7T GE/Agilent MR901, in the University of Ottawa pre-clinical imaging core. DCE-MRI was performed using a TRICKS sequence, with TE=1.1 ms, TR=4.3 ms, flip=30 deg, BW=83 kHz, FOV=7 cm, thick=2.4 mm, # of transverse slices=16, matrix=128x128, phase FOV=0.5, freq A/P, tempres=1.4 s, scan time 82 s, bolus i.v. 0.1 mmol/kg Gadovist (Bayer) diluted to 500 μL. Relative enhancement curves were analyzed with OLEA Sphere (Olea Medical). The AIF was determined automatically, then normalized to the venous output function.
Linear mixed effects modeling was used to analyze the data, including a metric for repeated measurements.
Results
Blood work (Fig 3). The CAF diet successfully generated several symptoms of metabolic syndrome.
MRI (Fig 4). Cerebral blood flow was significantly reduced following 2VO, with no effect of diet or time and no interaction (a). Cerebral blood volume in hippocampus was significantly reduced following 2VO, with no effect of time (b). In anterior brain, blood volume was also reduced after 2VO, in addition to a diet x time interaction at 14 weeks, wherein CAF animals had lower volume than SDs (c). A surgery x diet interaction was detected, wherein CAF animals had lower volume within the Sham group (d).
Behaviour (Fig 5). Diet or 2VO did not impact spontaneous locomotion, exploratory behaviour, object placement, context, or novel object tests (data not shown). In the water maze, there was no effect of diet or surgery on acquisition latency, distance, or swim velocity (a-c). However, animals in the CAF group spent significantly less time in the water maze target quadrant during the probe test than SD, indicating memory retention problems (d).
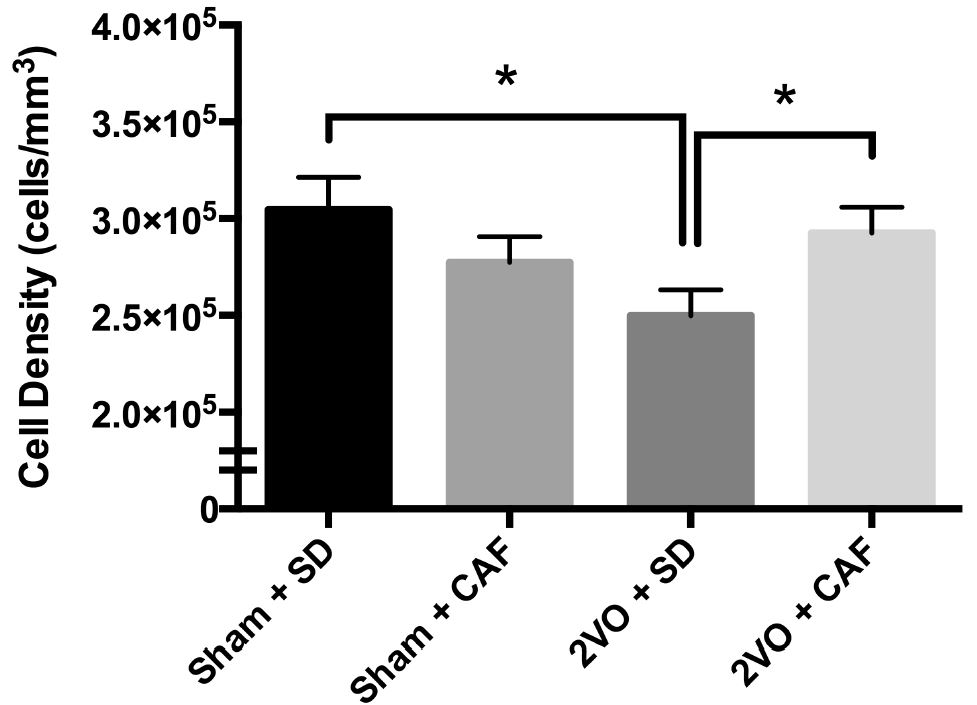
Histology (Fig 6). 2VO rats exhibited a significant reduction in corpus callosum volume (data not shown). For CA1 density, there was no effect of surgery, diet, or time; however, a significant surgery x diet interaction was detected. Post hoc analysis revealed that within the SD group, 2VO animals exhibited a significantly lower cell density versus Shams. Intriguingly, within the 2VO group, cell density in the CAF group was higher than the SD animals.
Discussion
In this study, two conditions commonly comorbid in cardiovascular disease (metabolic syndrome + cerebral hypoperfusion) were combined in a rat model to investigate the resulting neurological and physiological effects. This resulted in diet-induced metabolic syndrome with memory impairment, reduced blood flow and volume, white matter loss, and hippocampus cell density loss following global ischemia. The most striking effect of 2VO surgery was atrophy of the white matter, with a notable reduction in the volume of the corpus callosum. Furthermore, there was an intriguing increase in CA1 cell density within the 2VO animals that consumed Cafeteria diet, that warrants further exploration.Conclusion
We have successfully developed a clinically relevant rat model of comorbid VCI and metabolic syndrome. Our data suggest that these two conditions interact to produce differential effects, which may prove more useful in evaluating potential treatments for cardiovascular disease.Acknowledgements
The authors would like to thank Tara Read for help with the analysis; and W. Dale Stevens and Mariana Gomez-Smith for helpful discussions.References
1. Roth GA, Forouzanfar MH, Moran AE, Barber R, Nguyen G, Feigin V, Naghavi M, Mensah GA, Murray CJL: Demographic and Epidemiologic Drivers of Global Cardiovascular Mortality. N Engl J Med 2015, 372:1333–1341.
2. Yata K, Tomimoto H: Chronic cerebral hypoperfusion and dementia. Neurol Clin Neurosci 2014, 2:129–134.
3. Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit J a, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS, et al.: Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation 2011, 123:e18–e209.
4. Park Y-W, Zhu S, Palaniappan L, Heshka S, Carnethon MR, Heymsfield SB: The Metabolic Syndrome: Prevalence and Associated Risk Factor Findings in the US Population From the Third National Health and Nutrition Examination Survey, 1988-1994. Arch Intern Med 2003, 163:427–436.
5. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, Smith Jr. SC: Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International . Circulation 2009, 120:1640–1645.
6. O’Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp BH, Howells DW: 1,026 Experimental Treatments in Acute Stroke. Ann Neurol 2006, 59:467–477.
7. Perrin S: Make mouse studies work. Nature 2014, 507:423–425.
8. Fisher M, Feuerstein G, Howells DW, Hurn PD, Kent TA, Savitz SI, Lo EH: Update of the stroke therapy academic industry roundtable preclinical recommendations. Stroke 2009, 40:2244–2250.
9. Endres M, Engelhardt B, Koistinaho J, Lindvall O, Meairs S, Mohr JP, Planas A, Rothwell N, Schwaninger M, Schwab ME, Vivien D, Wieloch T, Dirnagl U: Improving outcome after stroke: overcoming the translational roadblock. Cerebrovasc Dis 2008, 25:268–278.
10. Dirnagl U, Hakim A, MacLeod M, Fisher M, Howells D, Alan SM, Steinberg G, Planas A, Boltze J, Savitz S, Iadecola C, Meairs S: A concerted appeal for international cooperation in preclinical stroke research. Stroke 2013, 44:1754–1760.
11. Gomez-Smith M, Karthikeyan S, Jeffers MS, Thomason LA, Janik R, Stefanovic B, Corbett D: A Physiological Characterization of the Cafeteria Diet Model of Metabolic Syndrome in the Rat. Physiol Behav .
12. Sampey BP, Vanhoose AM, Winfield HM, Freemerman AJ, Muehlbauer MJ, Fueger PT, Newgard CB, Makowski L: Cafeteria diet is a robust model of human metabolic syndrome with liver and adipose inflammation: comparison to high-fat diet. Obesity (Silver Spring) 2011, 19:1109–17.
13. Higa TS, Spinola A V, Fonseca-alaniz MH, Sant F, Evangelista A: Comparison between cafeteria and high-fat diets in the induction of metabolic dysfunction in mice. 2014, 6:47–54.
14. Johnson AR, Wilkerson MD, Sampey BP, Troester M a, Hayes DN, Makowski L: Cafeteria diet-induced obesity causes oxidative damage in white adipose. Biochem Biophys Res Commun 2016, 473:545–550.
Figures
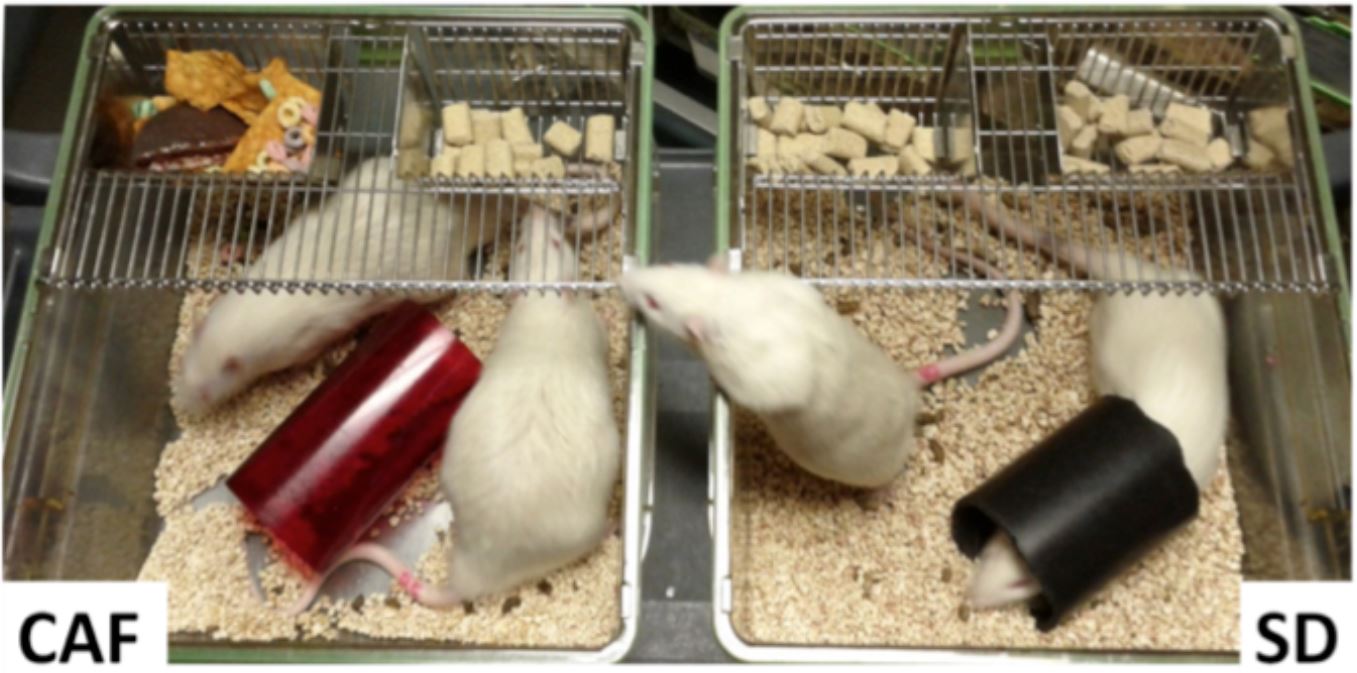
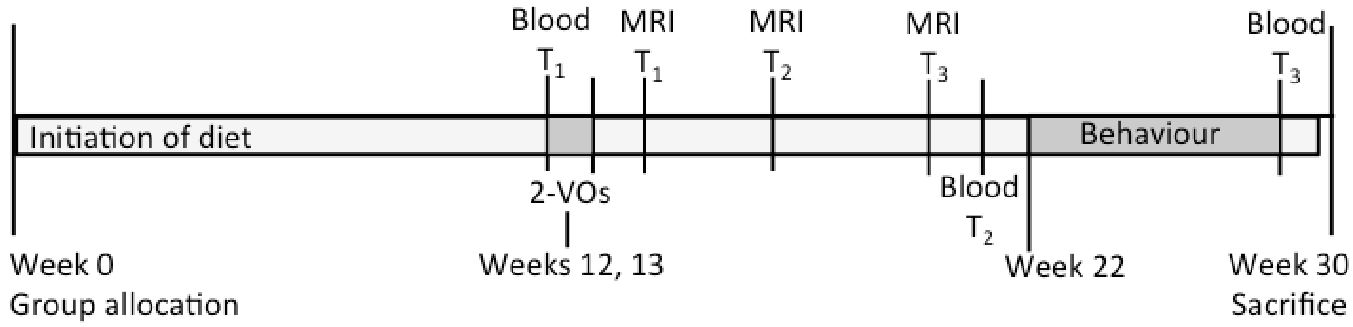
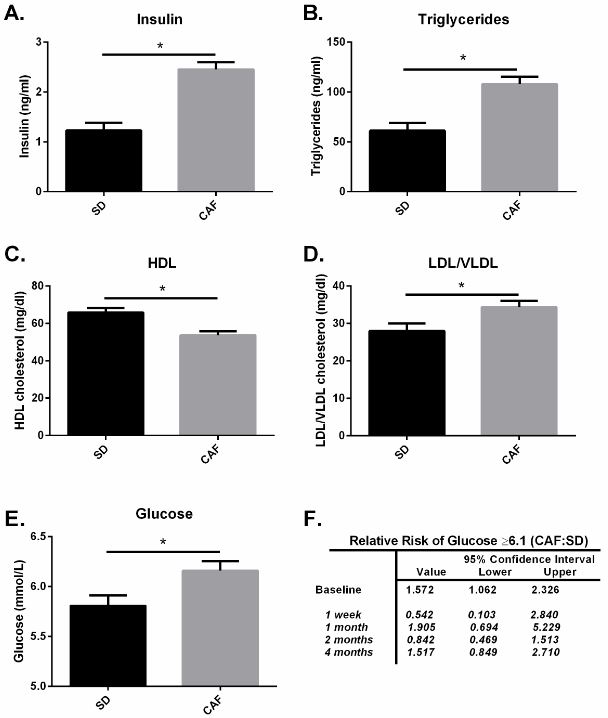
Fig 3. Metabolic data obtained from blood sampling. Values are mean +- SEM. The CAF diet successfully generated several symptoms of metabolic syndrome, including hyperinsulinemia (A), dyslipidemia (B-D), and increased fasted blood glucose (E-F).
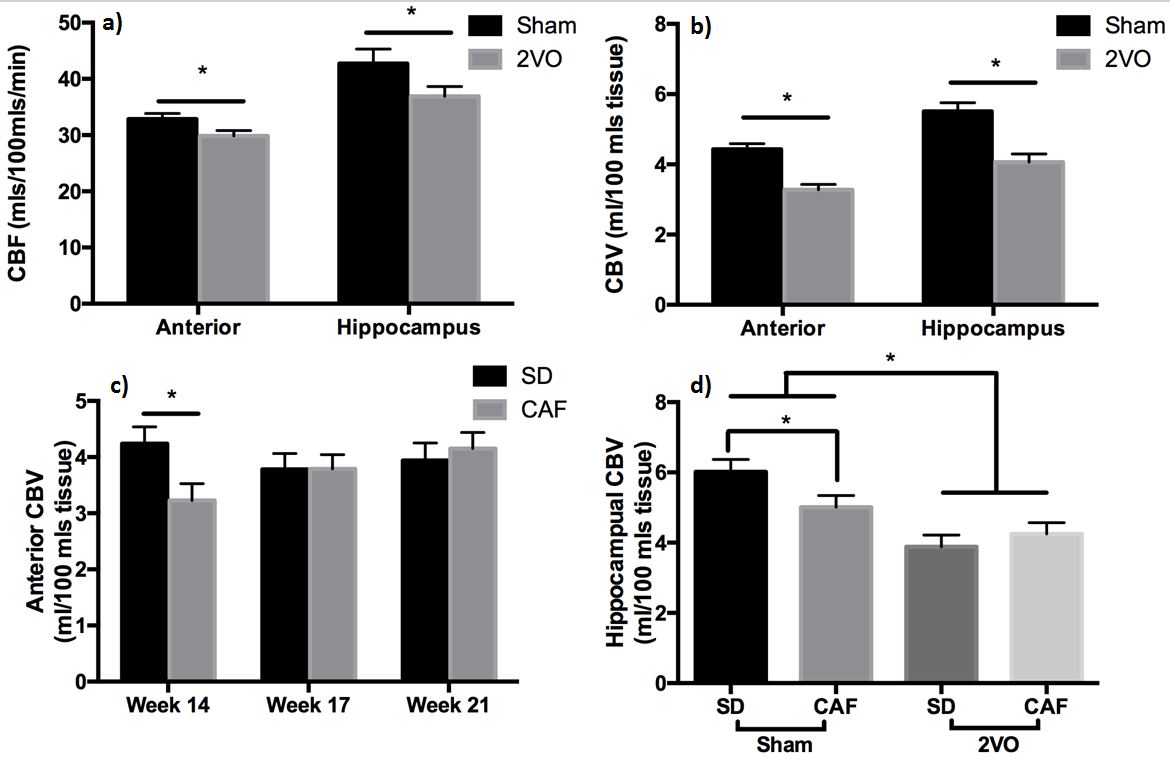
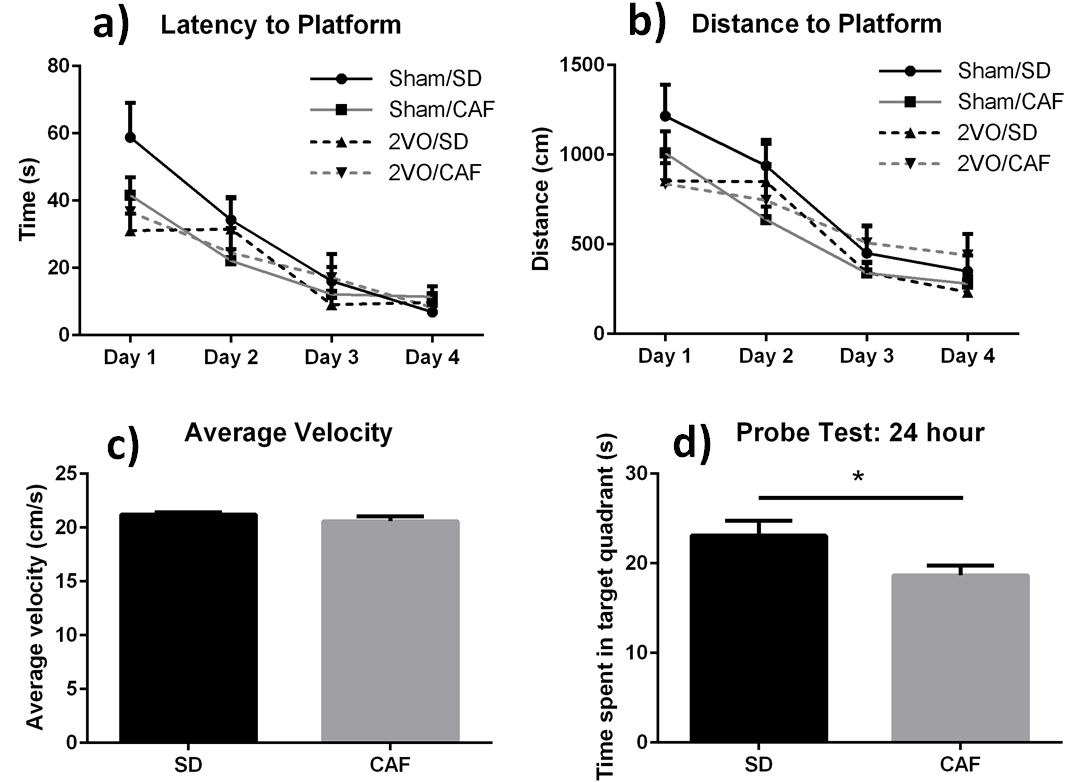
Fig 5. Morris Water Maze results. Values are mean +- SEM. a) Time required for the rat to find the submerged platform. b) Distance the rat swam before locating the platform. c) Average swim speed. d) After removing the platform, this is the time the rat spent in the quadrant that previously contained the escape platform. The more time spent in that quadrant, the better the rat's memory.