4065
Automated Lateral Ventricle Segmentation in Multiple Sclerosis – Assessing Reliability and Clinical Impact in a 5-Years Follow-Up Cohort Study1Medical Image Analysis Center AG, Basel, Switzerland, 2Department of Neurology, Universitätsspital Basel, Basel, Switzerland, 3Department of Neuroradiology, Universitätsspital Basel, Basel, Switzerland, 4Department of Neurology, University Hospital Düsseldorf, Düsseldorf, Germany, 5Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genoa and IRCCS S. Martino-IST, Genoa, Italy
Synopsis
As pars pro toto, lateral ventricle enlargement might give an indirect estimate of brain atrophy. In contrast to whole brain atrophy, ventricle enlargement is, however, clinically easy to assess and its quantification is robust to MR images of less than perfect quality. Here we investigate i) the applicability of an automatic lateral ventricle delineation algorithm (ALVIN) in multiple sclerosis (MS), and ii) the association between of lateral ventricle enlargement and clinical disability in MS longitudinally. We found that ALVIN reliably estimates the lateral ventricle volume in MS that is associated with whole brain atrophy and neurological as well as cognitive disability.
Introduction
As pars pro toto, lateral ventricle enlargement might give an indirect estimate of brain atrophy. In contrast to whole brain atrophy, ventricle enlargement is, however, clinically easy to assess and its quantification is robust to MR images of less than perfect quality. Here we investigate i) the applicability of an automatic lateral ventricle delineation algorithm (ALVIN) in multiple sclerosis (MS), and ii) the association between of lateral ventricle enlargement and clinical disability in MS longitudinally.Methods
In total, 127 patients with relapsing-remitting (n=101), secondary-progressive (n=22) or primary-progressive (n=4) MS with 5 years follow-up were derived from a longitudinal MS cohort on the phenotype-genotype characterization of MS. Brain MRI was obtained on a 1.5 Tesla MRI system (Magnetom Avanto, Siemens Medical Solutions). The brain MRI protocol included high-resolution three dimensional T1-weighted (T1w) magnetization prepared rapid gradient echo (MPRAGE, repetition time (TR) 2100ms, echo time (TE) 3.9ms, inversion time (TI) 1100ms, flip angle 15°, isotropic resolution of 1 mm3, acquisition time 9 minutes), and a pre-contrast double echo proton density- and T2-weighted sequence (axial, spatial resolution 0.98x0.98x3mm3). ALVIN1 was used to calculate the normalized lateral ventricle volume (LVV) in comparison to a manual segmentation by applying a binary mask to spatially normalized lesion-filled cerebrospinal fluid (CSF) segmented images. T1w hypointense and T2-weighted (T2w) hyperintense lesions were marked using Amira (Mercury Computer Systems Inc., Chelmsford, USA). Lesion filling was done by using “lesion_filling” as part of the FMRIB Software Library (FSL, version 5.0, Oxford, UK).2 To estimate normalized brain volume (NBV), SIENAX was applied.3, 4 Neurological and cognitive disability was assessed using the Expanded Disability Status Scale (EDSS),5 the Multiple Sclerosis Functional Composite (MSFC)6 and the Paced Auditory Serial Addition Test (PASAT).7 Finally, the scan-re-scan reliability was assessed by using a two way mixed intraclass correlation model of absolute agreements and single measures to calculate an intraclass correlation coefficient (ICC). Since all variables other than disease duration and age were not normally distributed, any associations between LVV or LVV change and clinical outcomes or NBV were investigated by using non-parametric Spearman correlation.Results
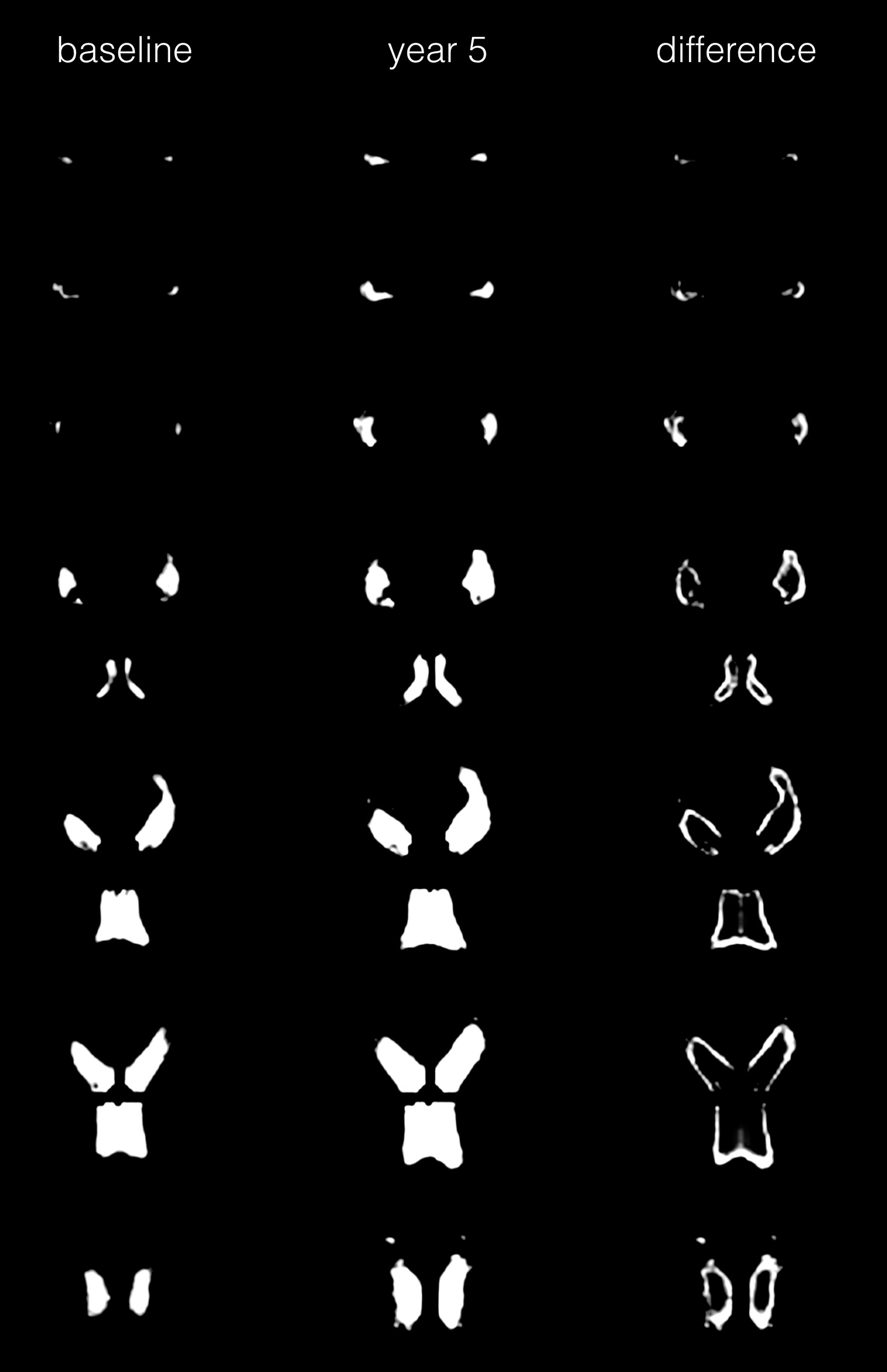
At baseline, mean LVV was 29.7±14.2 ml and correlated with age (rho=0.223, p=0.012), disease duration (rho=0.391, p<0.001), EDSS (rho=0.457, p<0.001), MSFC (rho=-0.451, p<0.001), PASAT (rho=-0.249, p=0.005), T1 lesion volume (rho=0.553, p< 0.001), T2 lesion volume (rho=0.558, p< 0.001) and NBV (rho=-0.591; p< 0.001). The agreement between ALVIN LVV and a manual lateral ventricle segmentation was high (intra-class correlation coefficient (ICC) = 0.991, mean difference 1.15±1.56 ml, range -5.3ml – 6.0ml). In addition, lateral ventricle enlargement was associated with an increase in T1w and T2w lesion volume, NBV reduction and a worsening of the PASAT score. In detail, the mean LVV increased by 3.6±4.6 ml over 5 years corresponding to a mean annual LVV change of 0.7 ml (2.4%, figure 1).Conclusion
ALVIN reliably estimates the LVV in MS that is associated with whole brain atrophy and neurological as well as cognitive disability.Acknowledgements
No acknowledgement found.References
1. Kempton MJ, Underwood TS, Brunton S, et al. A comprehensive testing protocol for MRI neuroanatomical segmentation techniques: Evaluation of a novel lateral ventricle segmentation method. Neuroimage 2011;58:1051-1059.
2. Battaglini M, Jenkinson M, De Stefano N. Evaluating and reducing the impact of white matter lesions on brain volume measurements. Hum Brain Mapp 2012;33:2062-2071.
3. Smith SM, Jenkinson M, Woolrich MW, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004;23 Suppl 1:S208-219.
4. Smith SM, Zhang Y, Jenkinson M, et al. Accurate, robust, and automated longitudinal and cross-sectional brain change analysis. Neuroimage 2002;17:479-489.
5. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983;33:1444-1452.
6. Fischer JS, Rudick RA, Cutter GR, Reingold SC. The Multiple Sclerosis Functional Composite Measure (MSFC): an integrated approach to MS clinical outcome assessment. National MS Society Clinical Outcomes Assessment Task Force. Mult Scler 1999;5:244-250.
7. Gronwall DM. Paced auditory serial-addition task: a measure of recovery from concussion. Percept Mot Skills 1977;44:367-373.
Figures