4013
Evaluation of Rapid Radial Imaging Methods for Assessment of First Pass Myocardial Perfusion1University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Rapid image acquisition is required to assess myocardial first-pass perfusion. K-t CS which uses compressed sensing has produced dynamic images with sufficient resolution. View sharing methods such as k-t VS could potentially provide similar results eliminating the need for regularization weights and significantly decreasing reconstruction time. K-t CS and k-t VS were investigated to determine their temporal and spatial response during first-pass myocardial perfusion. Results demonstrate that images reconstructed using each method had similar resolution and showed good correlation in assessing uptake kinetics. However, at higher acceleration, k-t CS showed increased SNR and smoother appearance while k-t VS used a less computationally intense and faster reconstruction.
Introduction
Rapid image acquisition with adequate temporal and spatial resolution to resolve uptake kinetics is required for myocardial dynamic first-pass perfusion. K-t compressed sensing (k-t CS) methods have demonstrated an ability to produce dynamic images with high spatial and temporal resolution and volumetric coverage [1,2]. K-space temporal view sharing methods (k-t VS) could potentially provide similar resolution and coverage without the need to determine regularization weights or the lengthy time required for reconstruction [3]. Here, we study whether k-t CS and k-t VS effectively use similar temporal weighing and will reconstruct images with comparable SNR and temporal and spatial resolution.Methods
Reconstruction methods, k-t CS and k-t VS were investigated to determine their temporal and spatial response during first-pass myocardial perfusion. An animal myocardial infarct model was used to assess the regional kinetic response for each reconstruction method. A total of six Dorset sheep were imaged at four-week post infarct where the uptake kinetics for the LV cavity, myocardium and remote region were determined using both reconstruction methods. Image data was acquired using a modified, prototypical saturation recovery spoiled gradient echo sequence with the following parameters: Golden angle k-space sampling (111.25o), FOV=300mm x 300mm, slice thickness = 8mm, flip angle = 10o TE=1.08ms, TR=1.75ms, bandwidth = 650Hz/pixel, TI = 35ms, repetitions = 60, spatial resolution = 2.3mm x 2.3mm, total radial projections = 1920. Golden-angle k-space acquisitions were reconstructed with k-t CS and k-t VS using both 32 and 16 projections, producing an effective temporal resolution of 56ms and 28ms respectively. Kinetic uptake curves for both methods were evaluated using Pearson Correlation and percent root-mean-squared-error (%RMSE). Comparisons were made between methods for LV cavity, myocardium and remote region kinetics. Uptake slope measured from the kinetic curves bounded by 20% above minimum signal and 20% below peak signal were compared for methods and regions.Results
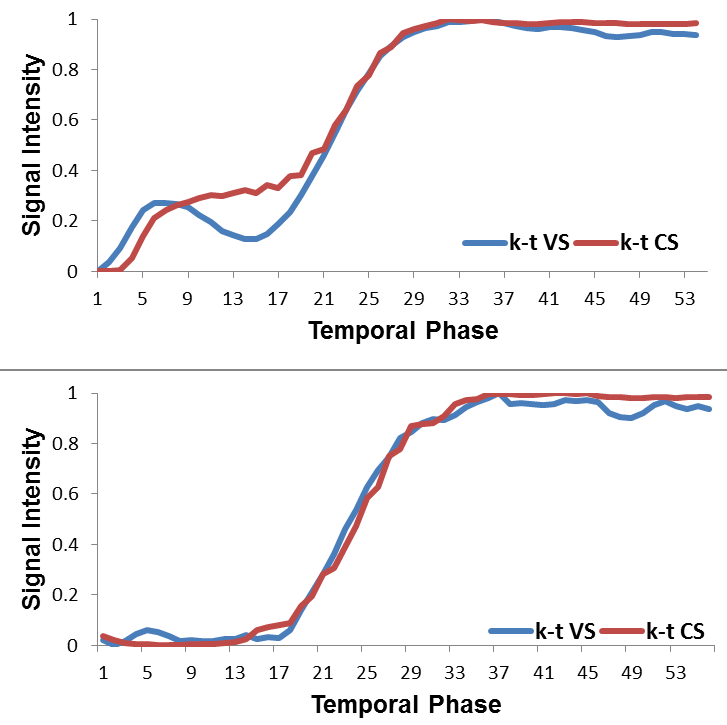
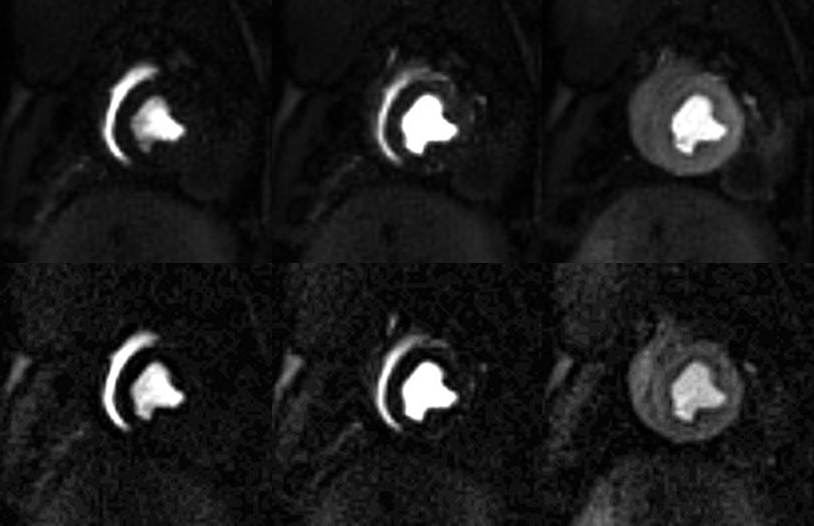
Representative images of first-perfusion reconstructed from 32 projections for both k-t CS and k-t VS are shown in Figure 1. Reconstruction of the single slice for k-t CS and k-t VS required 5.28 minutes and 0.056 minutes respectively. Image quality was similar for both reconstructions with comparable SNR and the absence of streak artifact. The myocardial wall is also well defined in both and peak signal enhancement equivalent. Regional perfusion kinetics curves show excellent agreement for the 32 projection k-t CS and k-t VS reconstruction (Figure 2). All regional curves had low %RMSE and significant correlation when comparing k-t CS and k-t VS reconstruction (%RMSE; Cavity 2.36%±0.46, myocardium 5.89%±1.3, remote 5.24%±1.4: R2; Cavity 0.99±0.002, myocardium 0.98±0.008, remote 0.98±0.01). Uptake slope measured over all regions for both methods indicated similar temporal response during maximum signal change (Cavity; k-t CS 0.15±0.03, k-t VS 0.13±0.04, myocardium; k-t CS 0.05±0.008, k-t VS 0.06±0.01, remote; k-t CS 0.11±0.05, k-t VS 0.12±0.04). To investigate increased acceleration, a subgroup was reconstructed using 16 projections. Image quality was enhanced with k-t CS compared to k-t VS with increased SNR and a smoother overall appearance (Figure 3). Delineation of myocardial wall was comparable and signal enhancement appeared consistent. Cavity kinetics curves where similar (%RMSE 3.47%± 0.4, R2 0.98±0.005) with k-t CS demonstrating a slightly greater uptake slope (k-t CS 0.18±0.5, k-t VS 0.15±0.03). %RMSE was slightly higher in the myocardium and remote curves (%RMSE; myocardium 6.90%±1.3%, remote 3.83%±0.4) due to increased image noise, while uptake slopes where comparable (myocardium; k-t CS 0.07±0.001, k-t VS 0.07±0.01, remote; k-t CS 0.07±0.007, k-t VS 0.07±0.004).Conclusion
K-t VS and k-t CS are both effective in reconstructing high frame-rate images from dynamic golden angle radial acquisitions. Both methods are suitable for first-pass myocardial perfusion imaging. Images reconstructed using each method had similar resolution and showed good correlation in assessing uptake kinetics. However, at higher acceleration rates, k-t CS showed increased SNR and a smoother overall appearance while k-t VS used a less computationally intense and faster reconstruction.Acknowledgements
We acknowledge the work of Robert Grimm, Li Feng, Tobias Block and Ricardo Otazo of New York University in the development of the GRASP reconstructionsoftware.References
1. Otazo R, Kim D, Axel L, et al. Combination of Compressed Sensing and Parallel Imaging for Highly Accelerated First-Pass Cardiac Perfusion MRI. MRM 2010;64:767–776. 2. Feng L, Grimm R, Block KT, et al. Golden-Angle Radial Sparse Parallel MRI: Combination of Compressed Sensing, Parallel Imaging, and Golden-Angle Radial Sampling for Fast and Flexible Dynamic Volumetric MRI. MRM 2014;72:707–717. 3. Song HK, Dougherty L, Schnall MD. Simultaneous Acquisition of Multiple Resolution Images for Dynamic Contrast Enhanced Imaging of the Breast. MRM 2001;46:503–509.Figures