3995
Semi-Automated Assessment for Distinguishing Glioblastoma and Solitary Brain Metastasis: A Machine Learning Approach1Department of Radiology, Mount Sinai Medical Center, New York, NY, United States, 2Mount Sinai Medical Center, New York, NY, United States
Synopsis
Although machine learning applications for non-medical imaging are well-established, its use in radiologic imaging interpretation remains nascent. We trained a support vector machine using advanced MR imaging to differentiate glioblastoma and brain metastasis with 72.6% balanced accuracy. The ability for machine learning to aid radiologists in differentiating pathologies with similar appearance on conventional imaging appears promising.
Purpose
Differentiating glioblastoma and solitary brain metastasis in patients with an undiagnosed primary malignancy can be challenging using conventional MR imaging, however accuracy may be improved with the addition of MR diffusion and perfusion parameters 1,2. Recent advances in machine learning (ML) have demonstrated promising advances in enabling interpretation of multimodal imaging data to differentiate neoplastic processes within the brain 3,4. We investigate whether ML evaluation of multimodal MR can reliably differentiate glioblastoma from brain metastasis.Materials & Methods
Preoperative MR imaging including fluid attenuated inversion recovery (FLAIR), diffusion-weighted images (DWI), dynamic contrast enhanced (DCE), dynamic susceptibility contrast (DSC) perfusion and post-contrast T1 (T1C+) in patients with solitary enhancing lesions were retrospectively reviewed.
MR perfusion studies were first processed using commercially available FDA-approved software (Olea Sphere, Olea Medical SAS, La Ciotat, France). The arterial input function was selected automatically and multiparametric perfusion maps were calculated using an extended toft model5 for DCE and Bayesian probabilistic method for DSC6.
The relative cerebral blood volume (rCBV) and relative cerebral blood flow (rCBF) from DSC, volume transfer constant from plasma to extravascular extracellular space (EES) (Ktrans), rate constant between EES to plasma (Kep), plasma volume per unit tissue volume (Vp) and EES-volume per unit tissue volume (Ve) from DCE in addition to apparent diffusion coefficient (ADC) maps from DWI were calculated and exported from the software for subsequent analysis.
Conventional (T1C+, FLAIR) and above processed maps were then analyzed using the fMRI Software Library (Analysis Group, Oxford, UK) Version 5.0.7 Preprocessing steps included brain extraction, histogram normalization and coregistration. Adequacy of sequence coregistration was ensured using visual inspection for all cases. Two separate volumes of interest (VOIs) were drawn manually on enhancing tumor and non-enhancing T2 hyperintense (NET2) region using coregistered T1C+ and FLAIR images respectively.
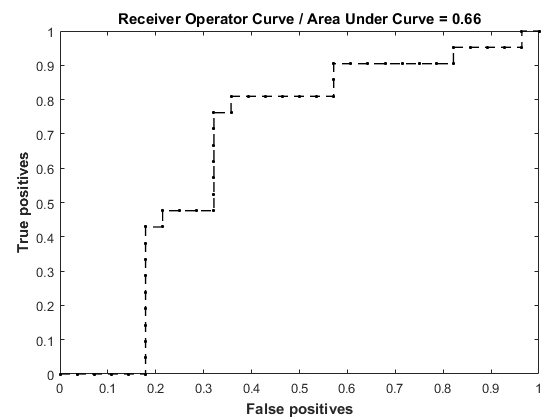
The preprocessed imaging data were utilized for supervised training of a ML classification kernel using the Pattern Recognition for Neuroimaging Toolbox (PRoNTo; University College London, London, UK) Version 2.0.8 Training entailed evaluation of labeled (i.e., glioblastoma vs. metastasis) MR imaging data for creation of a support vector machine kernel, which was validated on unlabeled cases using the leave-one-subject-out method. Quantitative analysis from VOIs (including ADC 10th percentile, rCBV 90th percentile, rCBF 90th percentile, ktrans 90th percentile, Kep 90th percentile, VP 90th percentile and Ve 90th percentile), ML balanced and class-specific accuracies, and receiver operating statistical data were collected. Balanced accuracy is a weighted composite of the individual accuracies obtained for each test case and is sensitive to any imbalance in the number of subjects in each classification group. Individual class accuracies are adjunctive measures that may reveal whether a trained model favors one class over another.
Results
Surgical pathology revealed glioblastoma in 7 patients and metastasis in 5 patients (lung carcinoma=2, esophageal carcinoma=1, melanoma=1, neuroendocrine carcinoma=1). Patient demographics included 7 males and 5 females with average age 52 ± 11 years. The trained ML kernel discriminated with 72.6% balanced accuracy (p=0.0001; 10,000 permutations) between glioblastoma [k1] (class accuracy 64.3%; p=0.28; 10,000 permutations) and metastasis (class accuracy 81.0%; p=0.004; 10,000 permutations), with the highest accuracy achieved from combined evaluation of ADC, rCBV, ktrans and VP using enhancement-based VOIs. Discrimination accuracy was decreased using NET2 VOIs, yielding 67.6% balanced accuracy (p=0.02; 1000 permutations) for glioblastoma (class accuracy 61.9%; p=0.35; 1000 permutations) and metastasis (class accuracy 73.3%; p=0.08; 1000 permutations).Discussion
As machine learning is embraced by radiologists and the larger medical community, we describe the application of training support vector machines to distinguish pathologies that may appear indiscernible on conventional imaging. Given a set of VOIs defined by lesional contrast enhancement, a trained support vector machine kernel can accurately differentiate between glioblastoma and brain metastasis utilizing ADC, rCBV, ktrans and VP. VOIs defined by perilesional NET2 yielded a support vector machine kernel with reduced accuracy. A larger prospective study is needed to validate our results.Conclusion
A trained support vector machine kernel can accurately differentiate between glioblastoma and brain metastasis utilizing ADC, rCBV, ktrans and VP within the enhancing component.Acknowledgements
None.References
1. Calli, Cem, et al. "Perfusion and diffusion MR imaging in enhancing malignant cerebral tumors." European journal of radiology 58.3 (2006): 394-403.
2. Svolos, Patricia, et al. "The role of diffusion and perfusion weighted imaging in the differential diagnosis of cerebral tumors: a review and future perspectives." Cancer Imaging 14.1 (2014): 1.
3. Goetz, Michael, et al. "Learning from small amounts of labeled data in a brain tumor classification task." Second Workshop on Transfer and Multi-Task Learning: Theory meets Practice, Montreal, Canada. 2014.
4. Zacharaki, Evangelia I., et al. "Classification of brain tumor type and grade using MRI texture and shape in a machine learning scheme." Magnetic Resonance in Medicine 62.6 (2009): 1609-1618.
5. Patlak, Clifford S., and Ronald G. Blasberg. "Graphical evaluation of blood-to-brain transfer constants from multiple-time uptake data. Generalizations." Journal of Cerebral Blood Flow & Metabolism 5.4 (1985): 584-590.
6. Boutelier, Timothé, et al. "Bayesian hemodynamic parameter estimation by bolus tracking perfusion weighted imaging." IEEE transactions on medical imaging 31.7 (2012): 1381-1395.
7. M.W. Woolrich, S. Jbabdi, B. Patenaude, M. Chappell, S. Makni, T. Behrens, C. Beckmann, M. Jenkinson, S.M. Smith. Bayesian analysis of neuroimaging data in FSL. NeuroImage, 45:S173-86, 200
8. J. Schrou, M. J. Rosa, J. M. Rodina, A. F. Marquand, C. Chu, J. Ashburner, C. Phillips, J. Richiardi, and J. Mourao-Miranda. PRoNTo: Pattern Recognition for Neuroimaging Toolbox. Neuroinformatics, 11(3):319{337, 2013.
Figures