3987
Performance comparison of artificial neural network and fuzzy deep learning algorithms for respiratory motion prediction in pseudocontinuous arterial spin labeling of the abdomen1Radiation Oncology and Radiology, Washington University in St Louis, St Louis, MO, United States, 2Imaging Physics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 3Electrical and Computer Engineering, Virginia Commonwealth University, Richmond, VA, United States, 4Radiation Oncology, University of California Los Angeles, Los Angeles, CA, United States, 5Medicine, University of Hawai'i at Manoa, Honolulu, HI, United States, 6High-Field Magnetic Resonance Center, Max Planck Institute for Biological Cybernetics, Tubingen, Germany, 7Biostatistics and Medicine, Washington University in St Louis, St Louis, MO, United States
Synopsis
Subtraction-based imaging methods like pseudocontinuous arterial spin labeling (pCASL) in the body are challenging due to physiological motion. Respiratory motion prediction (RMP) using an artificial neural network (ANN) and pencil beam navigators was previously integrated into a pCASL sequence to permit free-breathing perfusion MRI of the kidney. In an effort to improve the accuracy of the RMP, we compared the performance of a promising fuzzy deep learning (FDL) algorithm with ANN using navigator-echo displacements recorded from 8 volunteers during pCASL. FDL combines ANN with fuzzy logic. However, the ANN performance was significantly better than FDL for the pCASL application.
Purpose
Respiratory motion prediction (RMP) using an artificial neural network (ANN) was previously integrated into a pseudocontinuous arterial spin labeling (pCASL) sequence to permit free-breathing perfusion MRI of the kidney.1 The fuzzy deep learning (FDL) algorithm showed superior prediction performance to ANN in an earlier study using continuously sampled motion data with a short latency.2,3 FDL combines features of fuzzy logic with an ANN with two hidden layers. FDL potentially requires fewer prediction parameters and shorter computation times than ANN. In an effort to improve the performance of the RMP, we compared the performance of FDL with ANN for pCASL.Methods
Spiral pencil beam navigators were integrated into a pCASL sequence and executed every 100 ms during the RMP training period, the pCASL transit delay, and the extended “TR Fill” immediately following the multislice 2D EPI acquisitions (Fig. 1). The RMP training period consisted of 60 s of navigator acquisitions followed by a 20 s delay to permit the algorithm to calculate the optimal parameters. The TR Fill was lengthened specifically for the performance assessment of the RMP algorithms. The diaphragm/lung displacements from the navigators were input into the RMP algorithms.
Navigator echo data from the previous 8 volunteer scans performed on a Siemens 3T mMR (PET/MRI) were used for this simulation study. The pulse sequence and ANN algorithm was implemented in IDEA/ICE version VB20. A three-layer ANN was implemented with 15 input, 10 hidden, and 7 output nodes, respectively. ANN predictions were acquired in real-time during the MRI exam and logged. However, for the purpose of this study, we recalculated the predictions using the ICE simulator since some of the MRI log files were incompletely saved. There was no significant difference between the real-time and simulated ANN predictions.
FDL was simulated only in Matlab with 9 membership function, 6 linear regression, and 3 weight parameters. Thus, we were not able to compare computation times for the two algorithms since ANN was implemented in C++. The FDL algorithm produced a single prediction from the input navigator displacements. Therefore, the code was executed 7 times, each time with a different latency to cover the desired prediction window.
For both algorithms, the prediction performance was calculated using only the TR Fill navigator echoes and a moving window with the same length as the transit delay (15 navigators) to produce 7 time-equidistant predictions covering the 0.7 s image acquisition period. The prediction errors were calculated by using the successive navigator-echo measurements occurring after the window’s input displacements. The calculation was reperformed by incrementally moving the window forward in time, each time producing another 7 predictions until the end of the TR fill time was encountered.
Results
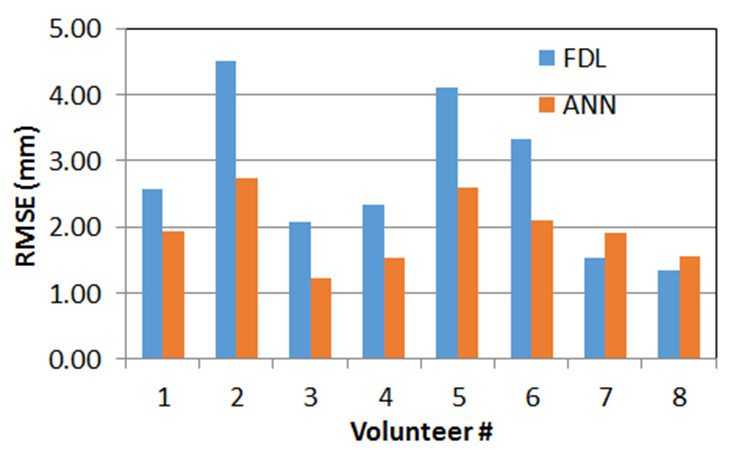
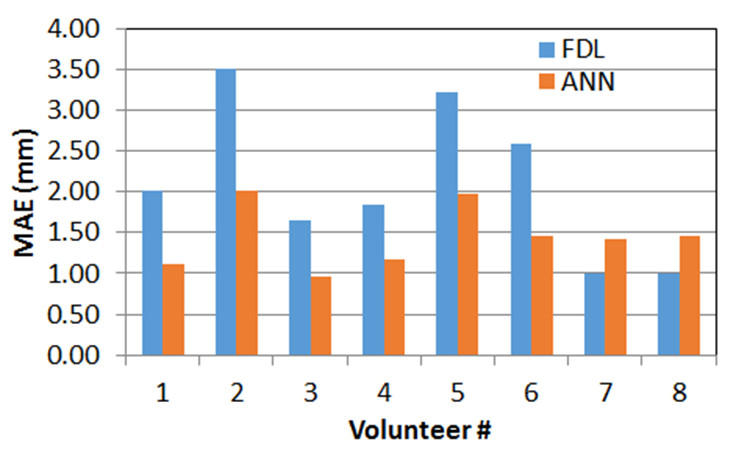
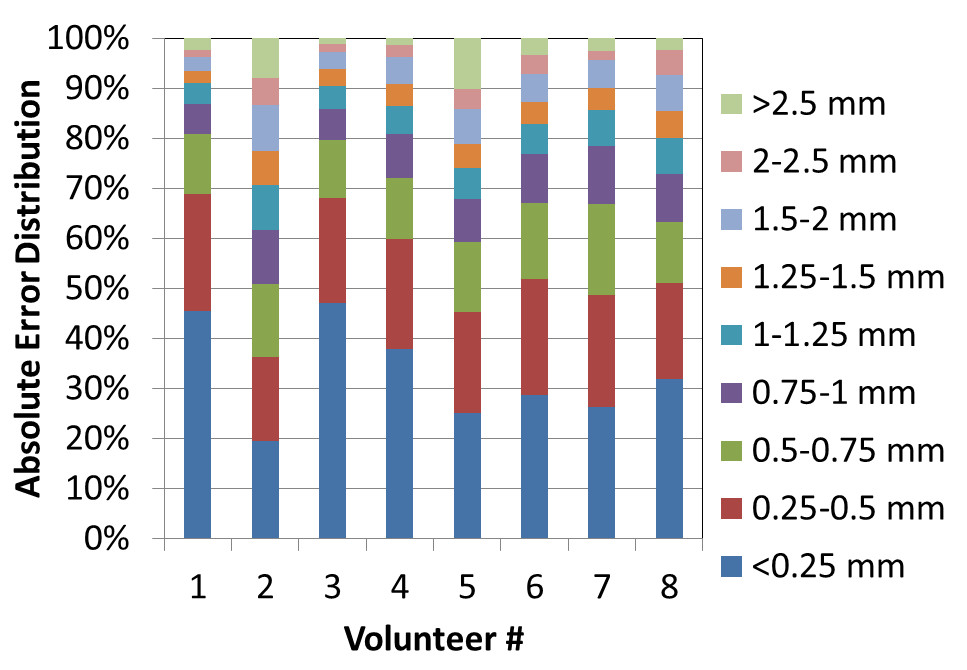
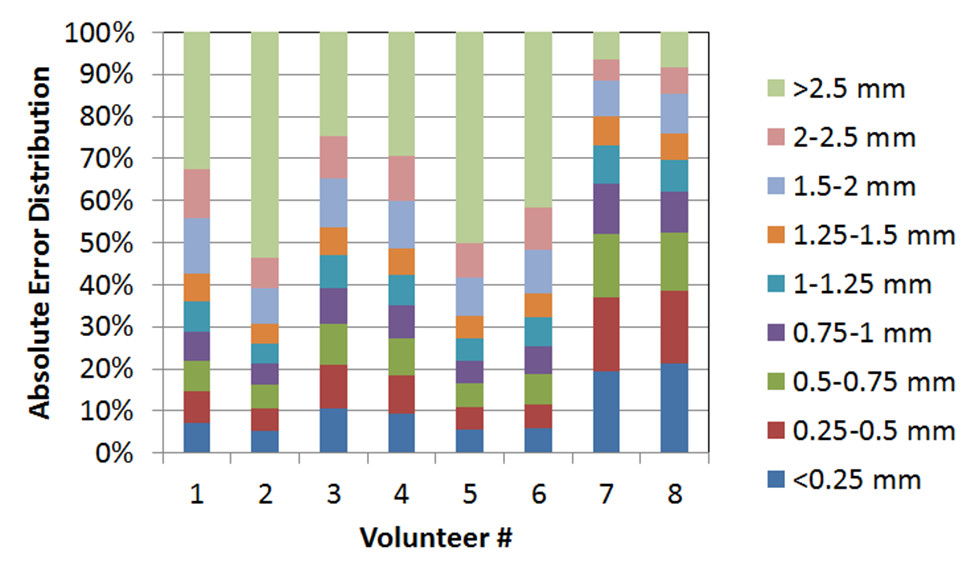
The root mean square error (RMSE) and mean absolute error (MAE) for the 8 volunteers were 1.91 ± 0.17 mm and 1.43 ± 0.17 mm, respectively, for the ANN. The overshoot was 23.58% ± 3.05% using the target prediction accuracy of ± 1 mm. The simulated RMSE and MAE for the FDL algorithm were 2.69 +/- 0.33 and 2.07 +/- 0.27 mm, respectively. The overshoot for FDL was 61.26% +/- 4.72%. A comparison of the RMSE and MAE results for each volunteer are shown in Figs. 2 and 3, respectively. The ANN clearly outperformed FDL for 6 of 8 volunteers. The absolute error distributions for ANN and FDL are shown in Figs. 4 and 5, respectively. ANN had a significantly higher fraction of small errors compared to FDL.Discussion
It should be noted that the FDL algorithm was not optimized for the pCASL application. The FDL algorithm used in this study was designed for continuous sampling and a single prediction (or latency). In contrast, the ANN was designed for multiple predictions for different latencies from the same input data. Hence, multiple FDL processes were required to generate the multiple predictions which would require either multi-threading on the MR image reconstruction (MRIR) computer or a different algorithm implementation.
The poorer performance of the FDL in this study versus the earlier study2 appears to be, in part, related to the longer latency associated with the pCASL application. Cyberknife respiratory motion data continuously sampled at 5-26 Hz were used in the original comparison of ANN and FDL.
Conclusions
The performance of the ANN was superior to that of the FDL in this study. As currently implemented, the FDL algorithm was not optimal for the pCASL-RMP application and timing. Further work is required to optimize the FDL method or find alternative RMP algorithms that produce smaller prediction errors than ANN for the perfusion application.Acknowledgements
This research was conducted primarily with the support of National Institutes of Health National Cancer Institute grant R01 CA159471 and National Science Foundation CAREER grant 1054333. Our research also received support from Washington University in St. Louis, The University of Texas MD Anderson Cancer Center, Virginia Commonwealth University, and UCLA.References
1) Song H, Liu W, Ruan D, Jung S, Gach HM. Free-breathing perfusion measurement using respiratory motion prediction. Proceedings of the 23st Annual Meeting of the ISMRM, Toronto, May 30-June 5, 2015.
2) Park S, Lee SJ, Weiss E., Motai Y, Intra- and inter-fractional variation prediction of lung tumors using fuzzy deep learning. IEEE J Transl Eng Health Med. 4:1-12 (2016).
3) Bagher-Ebadian H, Nagaraja TN, Paudyal R, Whitton P, Panda S, Fenstermacher JD, Ewing JR, MRI estimation of contrast agent concentration in tissue using a neural network approach. MRM 58(2):290-297 (2011).
Figures