3954
Simultaneous Variable-slab Dual-echo TOF MR Angiography and Susceptibility-Weighted Imaging1Dept. of Bio and Brain Engineering, KAIST, Daejeon, Korea, Republic of, 2Dept. of Radiology, Seoul National University Hospital, Seoul, Korea, Republic of, 3Dept. of Bio and Brain Enginnering, KAIST, Daejeon, Korea, Republic of
Synopsis
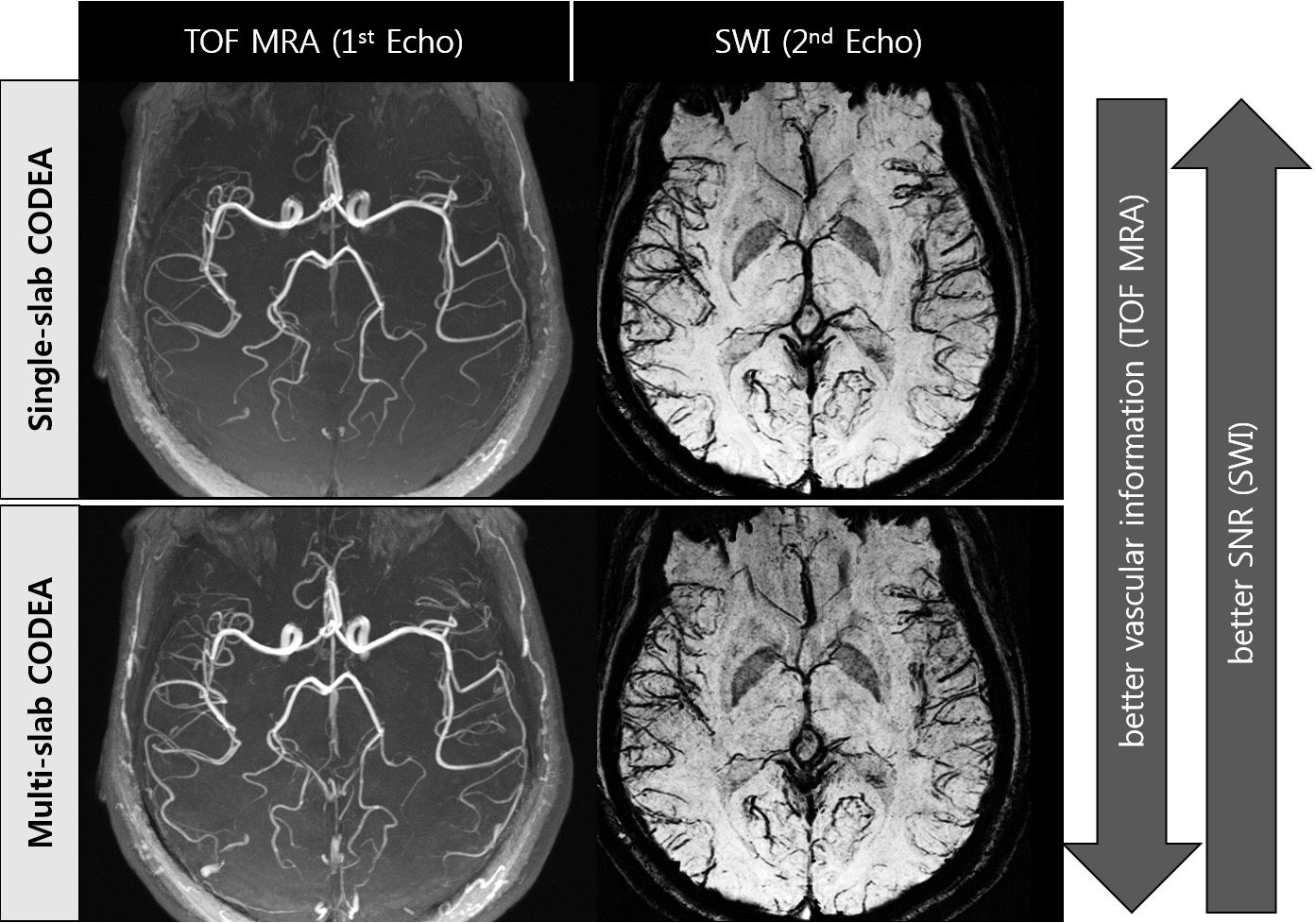
Multi-slab time of flight MR angiogram (TOF MRA) provides more detailed vascular structure than single-slab MRA, whereas single-slab susceptibility weighed imaging (SWI) provides better SNR than multi-slab SWI. In previous CODEA study, conflicting requirement on number of slab was not solved. In this study, we proposed and demonstrated an efficient method to acquire TOF MRA and SWI simultaneously with different number of slabs using variable-slab CODEA, which suppressed slab boundary artifacts in TOF MRA. Also demonstrated was acceleration of the variable-slab CODEA with a parallel imaging technique, GRAPPA. These improvements would provide more diverse clinical information in a limited scan time.
Purpose
To show feasibility of simultaneous 3D variable-slab dual-echo time‑of‑flight MR angiography (TOF MRA) and susceptibility weighed imaging (SWI) in combination with parallel imaging.Introduction
Compatible dual-echo arteriovenography (CODEA) was introduced for simultaneous acquisition of TOF MRA and SWI in optimal scan conditions by implementing two different optimal RF pulses in a one sequence [1-3]. For TOF MRA, multi‑slab imaging is generally preferred to single‑slab imaging because of better depiction of small arteries. For SWI, however, multi‑slab imaging is not desirable because of lower SNR (Fig.1). In the previous CODEA approaches the conflicting requirement on number of slabs was not resolved and feasibility of acceleration of data acquisition was not demonstrated. In this study, an advanced CODEA sequence is proposed for simultaneous acquisition of TOF MRA and SWI with different numbers of slabs for the dual echoes (variable-slab CODEA) and for acceleration of the proposed sequence with parallel imaging.Methods
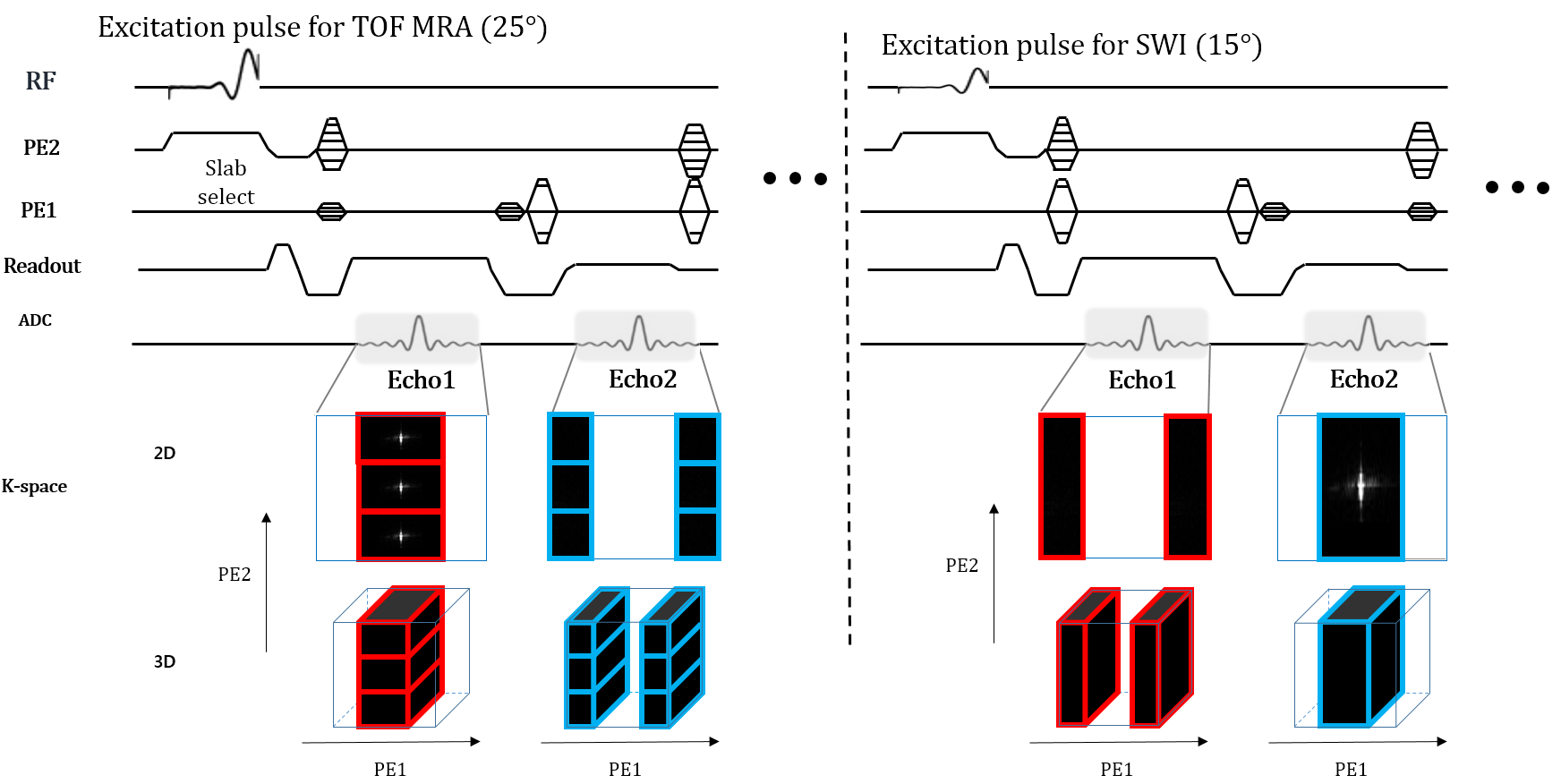
All data was acquired in 3T Siemens Trio MRI scanner with a 12-channel head coil. Two normal volunteers were scanned for this experiment. CODEA sequence was implemented by combining a dual-echo GRE sequence and the echo specific k-space reordering scheme applied along the first PE direction [1-3]. Imaging parameters of single-slab CODEA sequence were: TR=45ms, TE1/TE2=3.69/25ms, BW1/BW2=150/50 Hz/pixel, matrix size=384X192X72, FoV=240X180X72mm3, slice oversampling=33%, slice partial Fourier=6/8 and flip angle=25°/15°. Pre-saturation pulses and ramped RF pulses were used for TOF MRA in the first half of the acquisition, whereas flat regular RF pulses was used for SWI in the last half of the acquisition. Multi-slab CODEA was also performed with the same imaging parameters as the single-slab CODEA except acquisition with three overlapping slabs instead of a single slab. Imaging parameters of the variable‑slab CODEA were also the same as those of the single and multi-slab CODEA, however low and high frequency components were acquired with different slab numbers. When RF pulses for TOF MRA were used in the first half, three overlapping slabs were excited separately and sequentially. When RF pulse for SWI was applied in the second half, the whole single slab was excited for data acquisition (Fig.2).
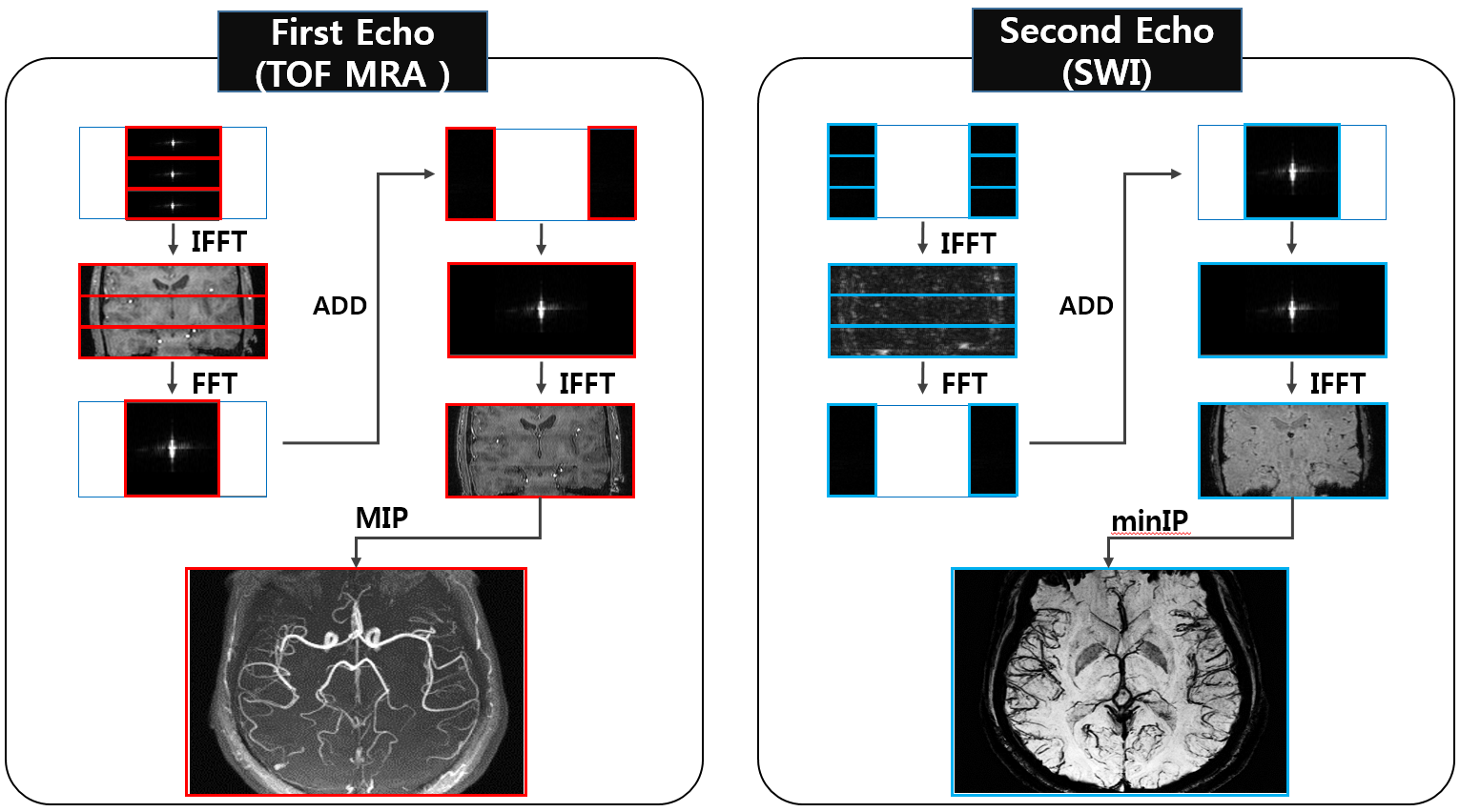
For the reconstruction of variable-slab CODEA, the low frequency component of the first echo and the high frequency component of the second echo were Fourier transformed into images separately for each of the three slabs. Each image was spatially stacked and transformed back to k-space domain to be combined with the high and low frequency components of the first and second echoes acquired with the single slab. They were then Fourier transformed again for final images (Fig.3). In order to implement parallel imaging, we down-sampled the data by a half (R=2) along the first PE direction with 18 reference lines. The down-sampled data were reconstructed with the GRAPPA algorithm [4]. Total scan time of the CODEA sequences without and with parallel imaging was 9 min and 5 min, respectively.
Results and Discussions
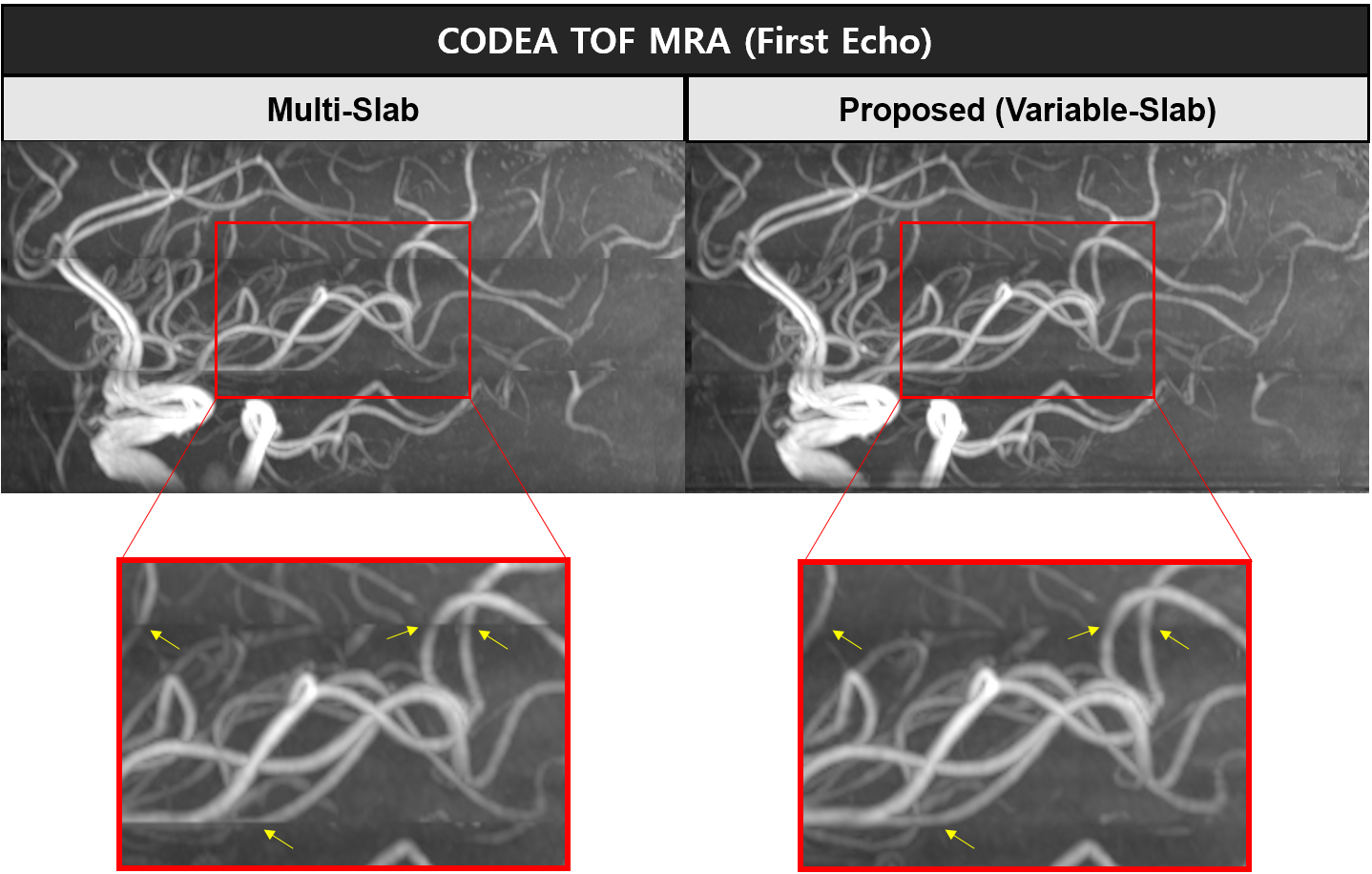
As shown in Fig.4, the proposed method provided optimal TOF MRA and SWI, which were visually similar to multi-slab CODEA TOF MRA and single-slab CODEA SWI acquired separately. In multi-slab CODEA TOF MRA, slab boundary artifacts were detected in the sagittal and coronal images in some subjects, because of motion and/or an imperfect ramp RF pulse profile. The proposed variable-slab CODEA method improved vessel connectivity at slab boundaries of TOF MRA compared to the multi-slab CODEA method, because high frequency components were acquired as a single slab in the whole region of interest (Fig.5). The improvement in vessel connectivity enables more accurate diagnosis and can be applicable to any multi-slab imaging including conventional TOF MRA with multiple overlapping slabs. Parallel imaging was successfully applied to the proposed method, reducing the scan time by half with slight reduction in image qualities (Fig.4). The image qualities may be further improved or higher acceleration factor may be applicable by optimizing parallel imaging algorithms or adopting compressed sensing algorithms in the future.Conclusion
The proposed variable-slab CODEA method enabled us to acquire multi-slab TOF MRA and single-slab SWI simultaneously. It could be combined with parallel imaging, reducing the scan time down to 5 min. It showed an additional benefit of suppressing slab boundary artifacts in the multi-slab TOF MRA through acquisition of high frequency components as a single whole slab. These improvements make CODEA more desirable for routine clinical application of simultaneous TOF MRA and SWI, providing more diverse clinical information in a limited scan time.Acknowledgements
No acknowledgement found.References
1. Park et al. MRM 2009;61:767-774
2. Park et al. MRM 2010;63:1404-1410
3. Do et al. MRM 2016;76:1504-1511
4. Griswold et al. MRM 47:1202-1210
Figures