3932
Self-gated 4D-MRI of the Liver: Initial Clinical Results of Comprehensive Real-Time Imaging of Hepatic Enhancement1Diagnostic and Interventional Radiology, University of Tuebingen, Tuebingen, Germany, 2Diagnostic and Interventional Radiology, University of Tuebingen, 3Section on Experimental Radiology, University of Tuebingen, 4Siemens Healthcare
Synopsis
A remaining challenge of abdominal MRI are artifacts due to patient motion. In this study, we evaluated a prototype volume-interpolated breath-hold examination (VIBE) sequence with automated respiration self-gating and compressed sensing reconstruction (VIBESG-CS) for continuous dynamic contrast-enhanced (DCE) liver MRI in comparison to a standard multiphase breath-hold examination (VIBEBH-STD). VIBESG-CS provided similar overall image quality and lesion conspicuity and improved image sharpness as compared to VIBEBH-STD. Therefore, VIBESG-CS seems to be a promising approach to improve the validity and reliability of DCE-MRI of the liver, especially in patients with impaired breath-hold capabilities.
Purpose
To evaluate the clinical application of self-gated (SG) free-breathing volume-interpolated breath-hold examination (VIBE) for continuous dynamic contrast-enhanced (DCE) MR imaging of the liver using Cartesian k-space sampling and compressed sensing (CS) reconstruction.Material and Methods
20
patients with hepatic pathologies underwent routine Gadobutrol-enhanced (Bayer
Healthcare, Germany) follow-up MRI of the liver at 1.5T (MAGNETOM Aera, Siemens
Healthcare, Erlangen, Germany). A prototypical self-gated free-breathing VIBE sequence
with Cartesian k-space sampling and CS reconstruction (VIBESG-CS) was
continuously acquired for 128 seconds starting with the administration of the
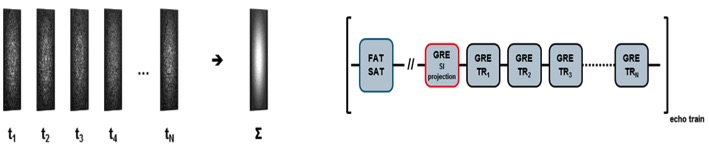
contrast agent. Relevant components of the acquisition are outlined in Figure
1. From the acquired raw data, 16 consecutive series (temporal resolution 8
seconds, spatial resolution of 1.2x1.2x3 mm) were reconstructed inline at the
scanner, using 40% of the data chosen by best consistency of the assigned
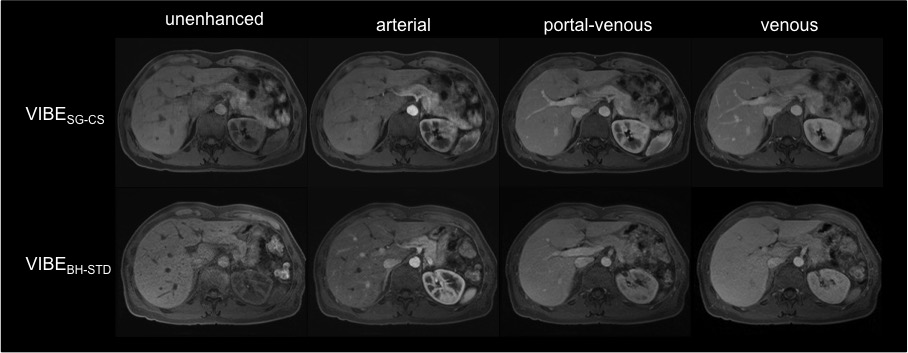
navigation signal. The unenhanced, arterial, portal-venous and venous phase
series were selected subjectively based on image quality for every patient and
compared to a conventional historical multiphase contrast-enhanced breath-hold
(BH) examination of the same patient used in clinical routine (VIBEBH-STD).
Image quality was assessed qualitatively (overall image quality, sharpness,
lesion conspicuity, vessel contrast, motion/other artifacts; two readers
independently; 5-point Likert scale; 5=excellent) and quantitatively
(coefficient-of-variation (CV); mean liver SI). Statistical analyses were
performed using SPSS (Version 22, IMB, USA). Wilcoxon signed-rank test was conducted
for the comparison of qualitative data. Paired t-test was performed for
quantitative measurements.Results
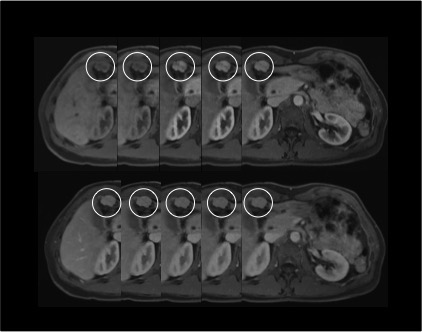
Overall image quality, lesion conspicuity and vessel contrast showed no significant differences between the sequences (p≥0.06, refer to Figure 2 and 3). Image sharpness was rated significantly higher in the arterial (4.0±0.7), portal-venous (4.4±0.6) and venous phase (4.4±0.6) images of VIBESG-CS as compared to VIBEBH-STD (3.5±0.7; 3.6±0.7 and 3.7±0.7, respectively; p≤0.03). No significant differences were found regarding motion artifacts (p≥0.07). However, VIBESG-CS showed a significant appearance of bow-like reconstruction artifacts most pronounced in the unenhanced series (3.4±0.8), followed by the arterial (3.7±0.7), portal-venous and venous phase images (both 4.0±0.6), which were not present in VIBEBH-STD (5.0±0.0; p=0.001). Mean liver SI was significantly higher in VIBEBH-STD (198.5±84.8) than in VIBESG-CS (171.7±63.5; p=0.002) whereas CV calculations revealed no significant differences between the sequences (p=0.1).Discussion
This
study indicates that VIBESG-CS is applicable for continuous
free-breathing DCE-MRI of the liver, providing similar image quality as
compared to a standard breath-hold sequence. This is of clinical interest,
especially in patients with impaired breath-hold capabilities, as artifacts due
to motion cause a considerable number of non-diagnostic examinations1. Moreover, exact timing of
the contrast agent bolus is crucial, to achieve an optimal arterial enhancement
pattern, which often remains challenging in clinical routine2.
This
issue can also be solved with the continuous data acquisition of VIBESG-CS, thus supporting the work of the technician and improving patient safety.
In this context,
free-breathing continuous data acquisition during the contrast agent passage
seems to be a helpful approach to improve the validity and reliability of DCE
liver MRI with potential implications for patient care. Furthermore, this
approach seems promising to allow for calculating quantitative perfusion
parameters as known from CT imaging, which provide additional information about
the perfusion characteristics of liver pathologies. Similar approaches have already
been reported using accelerated radial instead of Cartesian k-space sampling, which
also provided good image quality and reduced motion artifacts, however, at the
cost of a substantially prolonged reconstruction time, thus far limiting the
application in clinical routine3-5.Conclusion
VIBESG-CS is applicable for continuous free-breathing self-gated DCE-MRI of the liver at high temporal and spatial resolution providing similar overall image quality and lesion conspicuity and improved image sharpness as compared to VIBEBH-STD.Acknowledgements
No acknowledgement found.References
1. Reiner CS, Neville AM, Nazeer HK, et al. Contrast-enhanced free-breathing 3D T1-weighted gradient-echo sequence for hepatobiliary MRI in patients with breath-holding difficulties. Eur Radiol 2013;23(11):3087-3093.
2. Kazmierczak PM, Theisen D, Thierfelder KM, et al. Improved detection of hypervascular liver lesions with CAIPIRINHA-Dixon-TWIST-volume-interpolated breath-hold examination. Invest Radiol 2015;50(3):153-160.
3. Feng L, Axel L, Chandarana H, et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med 2016;75(2):775-788.
4. Chandarana H, Feng L, Block TK, et al. Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Invest Radiol 2013;48(1):10-16.
5. Chandarana H, Feng L, Ream J, et al. Respiratory Motion-Resolved Compressed Sensing Reconstruction of Free-Breathing Radial Acquisition for Dynamic Liver Magnetic Resonance Imaging. Invest Radiol 2015;50(11):749–756.
Figures