3927
Method of choice to increase the motion-robustness for free-breathing applications: Self-gating, motion-weighting, or extra-dimensional reconstruction1Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University School of Medicine, New York, NY, United States, 2Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University School of Medicine, New York, NY, United States
Synopsis
Previously proposed techniques based on non-Cartesian or modified Cartesian sampling schemes allow for free-breathing acquisitions with solid motion-robustness. However, residual artifacts such as motion blurring often remain. Techniques including self-gating, motion-weighting, and extra-dimensional reconstruction have been proposed to further improve image quality.
Here, an analysis of these techniques is provided by performing multiple reconstructions of several volunteer and patient datasets, which were then evaluated by radiologists.
Purpose
MRI of motion-sensitive applications such as abdominal or cardiac examinations has relied on strict breath-holding. However, breath-holding can fail especially for sick, elderly, or pediatric patients, which can render image quality non-diagnostic.
To overcome this problem, several techniques have been developed that allow for free-breathing acquisitions. These methods are often based on non-Cartesian trajectories1,2 or modified Cartesian sampling schemes3,4. Due to the underlying trajectory design, these approaches inherently achieve solid motion-robustness. However, residual artifacts such as motion blurring often remain. To further improve image quality of free-breathing exams, approaches including self-gating, motion-weighting5, and extra-dimensional reconstruction (XD)6 have been proposed. So far, however, it remained unclear how the performance of the methods compares.
The purpose of this work is to provide an analysis by performing multiple reconstructions of several volunteer and patient datasets, which were then evaluated by radiologists.
Methods
Data acquisition
Ten subjects were scanned with IRB-approval on clinical 3T scanners (Magnetom Prisma and Skyra, Siemens Healthcare). Free-breathing DCE liver MRI was performed in five volunteers (age 34.8±12.9). 1222 radial projections were continuously acquired for 3:10 min, using a 3D radial golden-angle stack-of-stars trajectory with the following parameters: FOV = 350x350mm2, matrix size = 256x256, slice thickness = 5mm, acquired partitions = 48, TR/TE = 3.6/1.6ms. After 20s, contrast agent was injected while the scan continued.
Furthermore, five patients (age 65.6±9.5) were scanned during free-breathing without dynamic injection of contrast agent. Here, a RAVE (RAdial Volumetric Encoding) sequence was employed, which is based on a 3D stack-of-stars trajectory with bipolar multi-echo readout. 600 radial projections were acquired in 3:18 min, using parameters as follows: FOV = 350x350mm2, matrix size = 256x256, slice thickness = 3mm, acquired partitions = 52, TR = 6.31ms, TE1/2/3 = 1.41/3.01/4.61ms.
Image reconstruction
The volunteer DCE datasets were reconstructed with the iterative Golden-angle RAdial Sparse Parallel (GRASP) technique1, which performs a joint multi-coil compressed sensing reconstruction with temporal total variation as sparse regularizer. The patient multi-echo datasets were reconstructed with the Dixon RAdial Volumetric Encoding (Dixon-RAVE) framework2, which performs fat/water separation using a model-based approach.
To further improve motion-robustness, the three following techniques were implemented. For GRASP, the different methods were applied to each dynamic contrast frame, while for Dixon-RAVE they were applied to the entire dataset.
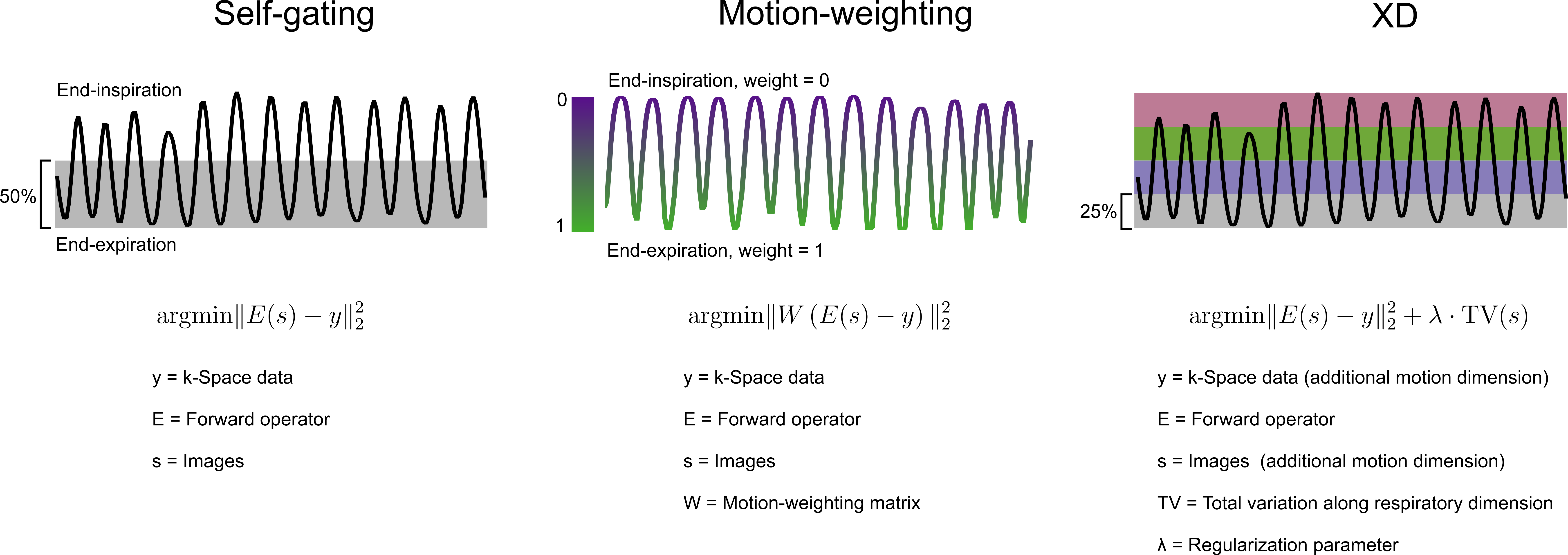
1) Self-gating, using an acceptance window of 50% starting from end-expiration.
2) Motion-weighted reconstruction, by weighting the data-fidelity term of the iterative optimization algorithm5 in the following way: The end-expiration state was considered motion-free and weighted with 1, while weights decreased exponentially with increasing distance on the respiratory curve3.
3) Extra-dimensional reconstruction (XD)6, by sorting data into four different respiratory states, ranging from end-expiration to end-inspiration. Undersampling artifacts of the different states were removed by minimizing total variation along this additional dimension to exploit sparsity between respiratory states.
Figure 1 shows implementation details and a schematic description of the different methods. The required motion estimate was extracted from k-space by computing the projection profiles, which were normalized and processed with a principal component analysis. Coil clustering7 was used to select the principal components which resemble respiration.
Reader evaluation
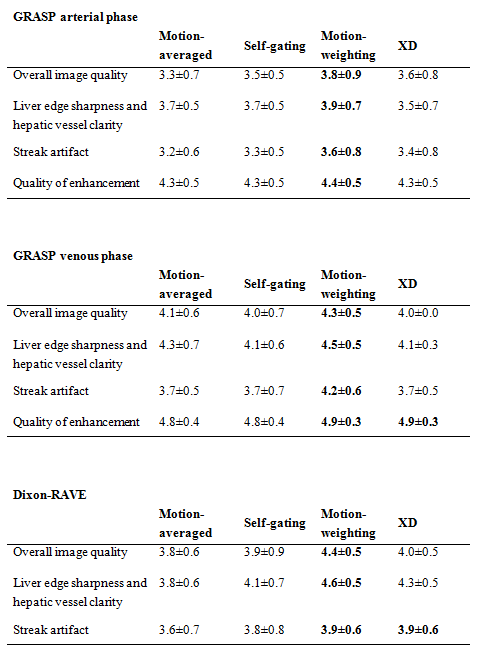
Images from the different techniques were pooled together in random order and rated by two blinded radiologists with 3/5 years of experience. For DCE datasets, arterial and venous phases were selected. In the XD reconstruction, the end-expiration image was chosen. The following metrics were scored on a 5-point scale: overall image quality, liver edge sharpness and hepatic vessel clarity, and streak artifact. For the GRASP datasets, quality of enhancement was scored as well. Mean and standard deviation were calculated for each technique.
Results
Figure 2 shows scores for the different techniques. When respiratory motion phases are appropriately weighted or separated in the reconstruction, higher scores are obtained in almost all categories compared to the motion-averaged results. Motion-weighting achieved the best scores for both GRASP and Dixon-RAVE.
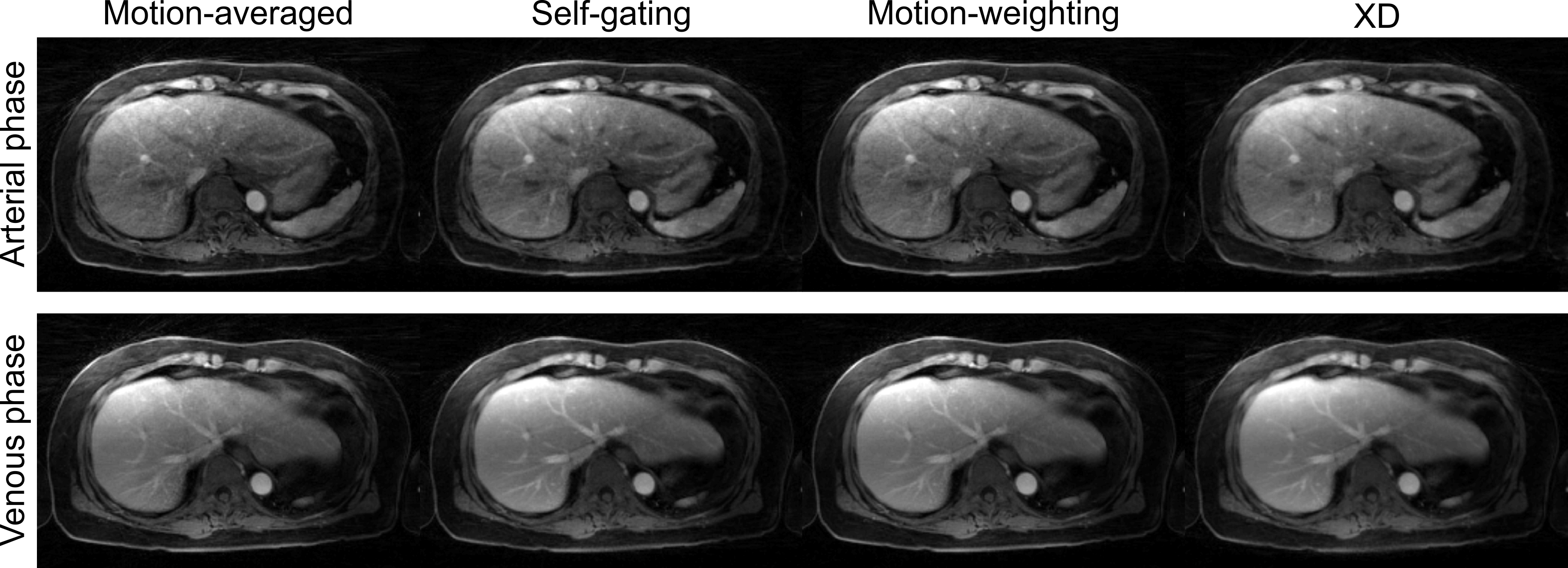
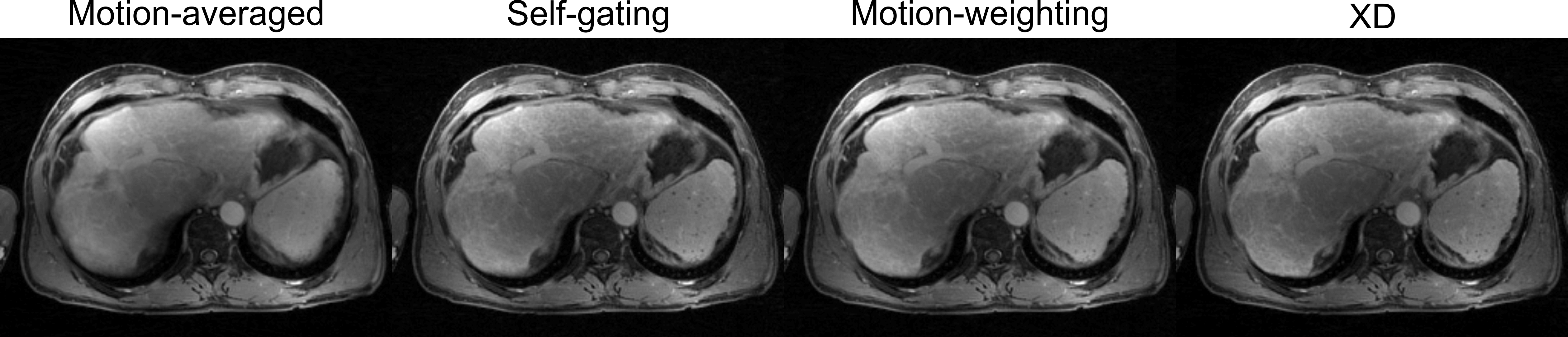
Results from the different reconstruction techniques applied on a DCE dataset are shown in Figure 3. Figure 4 shows corresponding results for a RAVE dataset.
Discussion and Conclusion
While self-gating only uses a reduced sampling efficiency (e.g., 50%), both motion-weighting and XD reconstruction use all of the acquired data. Overall, these more advanced techniques also achieved better results.
In summary, the best scores were obtained with motion-weighting which is, therefore, a well-suited method, in particular when only motion compensation is required for image diagnosis. However, when different respiratory phases have to be obtained, the XD approach is a valuable alternative.
Acknowledgements
NIH P41EB017183, 5R01EB018308References
1. Feng L et al., Golden-angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI, Magn Reson Med, 72:707-717 (2014)
2. Benkert T et al., Free-breathing volumetric fat/water separation by combining radial sampling, compressed sensing, and parallel imaging, Magn Reson Med, 10.1002/mrm.26392 (2016)
3. Cheng JY et al., Free-breathing pediatric MRI with nonrigid motion correction and acceleration, J Magn Reson Imag, 42:407-420 (2015)
4. Prieto C et al., Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step cartesian acquisition, J Magn Reson Imag, 41:738-746 (2015)
5. Johnson KM et al., Improved least squares MR image reconstruction using estimates of k-space data consistency, Magn Reson Med, 67:1600-1608 (2012)
6. Feng L et al., XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing, Magn Reson Med, 75:775-788 (2016)
7. Zhang T et al., Robust self-navigated body MRI using dense coil arrays, Magn Reson Med, 76:197-205 (2016)
Figures