3871
Real-time dynamic image reconstruction using Compressed Sensing and Principal Component Analysis (CS-PCA)1Oncology, University of Alberta, Edmonton, AB, Canada, 2Medical Physics, Cross Cancer Institute, Edmonton, AB, Canada
Synopsis
An online real-time reconstruction technique that combines compressed sensing with principal component analysis (CS-PCA) was developed for the purpose of adaptive radiotherapy using our Linac-MR system. Our technique uses a database of images, acquired prior to an incoherently accelerated acquisition, to fill in the missing lines of k-space using PCA. Our technique can reconstruct images ranging from 5-20 frames per second with minimal artefacts.
Purpose
Nearly one third of all cancer treatment involves the use of external beam radiotherapy (EBRT), which uses high energy photons delivered via a linear accelerator, or linac. Our study aimed to develop a real-time dynamic image reconstruction technique for the use in adaptive EBRT. Recently, our group has combined a linac and a bi-planar MRI into a single system known as the Linac-MR. In order to achieve real-time adaptive radiotherapy, an international task group has recommended a minimum system latency of 500 ms to acquire data, reconstruct the image, contour the region of interest (tumour), and deliver radiation1. Our study addresses the data acquisition and reconstruction step. We have developed a reconstruction algorithm that combines compressed sensing and principal component analysis (CS-PCA)2. The CS-PCA algorithm requires a database of fully sampled images, which are used to aid in the real-time reconstruction of incoherently under-sampled k-space data.Methods
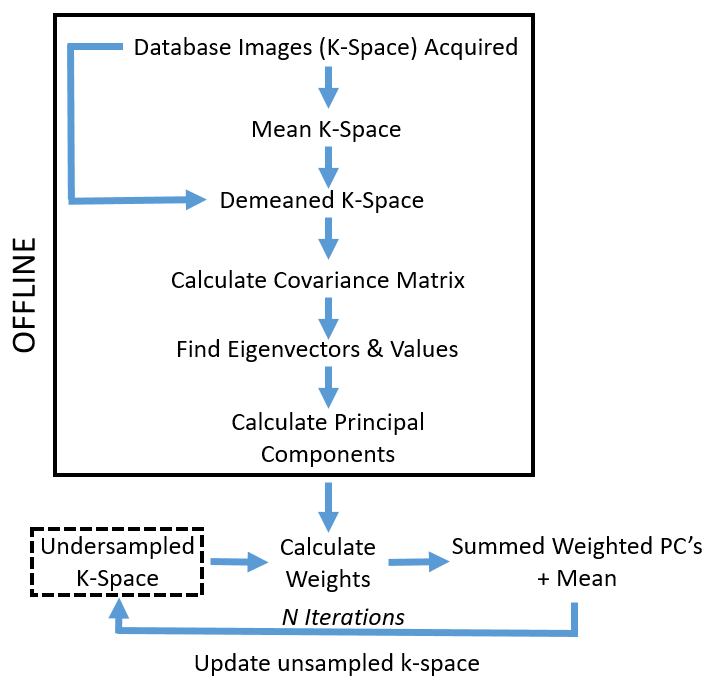
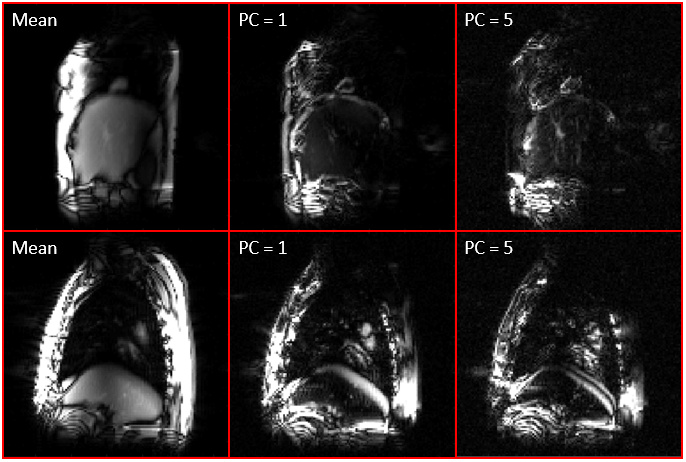
Six retrospective fully sampled dynamic data sets of patients with non-small cell lung cancer were used to investigate the CS-PCA algorithm. Fully sampled data was required as it allowed for a ground truth to compare tumour segmentation at different accelerations. The data sets were acquired at 3T and consisted of 650 free-breathing dynamic frames, acquired using a bSSFP pulse sequence (TE/TR = 1.1ms/2.2ms, FOV: 40x40cm2, 128x128). The CS-PCA algorithm is implemented in k-space and is shown schematically in Figure 1. Our CS-PCA implementation used a database of the initial 30 images, which were used to calculate the principal components (PCs) for reconstruction of the following 620 under-sampled images. The 620 images were incoherently under-sampled along the PE direction using a Monte Carlo based sampling scheme. The missing k-space data was calculated by projecting the current k-space data onto the PC's to generate the corresponding PC weights. The weighted PC's were summed together along with the mean database, and the missing k-space was iteratively updated. Figure 2 displays example mean database images, along with two (unweighted) PC's for two patients.
Acceleration factors ranging from 2-10x were investigated using both CS-PCA, and Split Bregman CS3. CS-PCA parameters were investigated and include the number of PCA iterations (updated PC weights per reconstruction), the PC threshold (dictates number of discarded PC's), and the database size. Metrics to determine the reconstruction quality include the artefact power (AP) and dice coefficients (DC) of the tumour segmentations. The DC compares the accelerated reconstruction contour to the fully sampled data contour for each image; a DC of 1 indicates a perfect segmentation. The contours are generated using a neural-network based segmentation algorithm4. As our Linac-MR system uses a 0.5T bi-planar magnet, simulated 0.5T images were generated by adding Gaussian noise to the 3T data sets5,6.
Results and Discussion
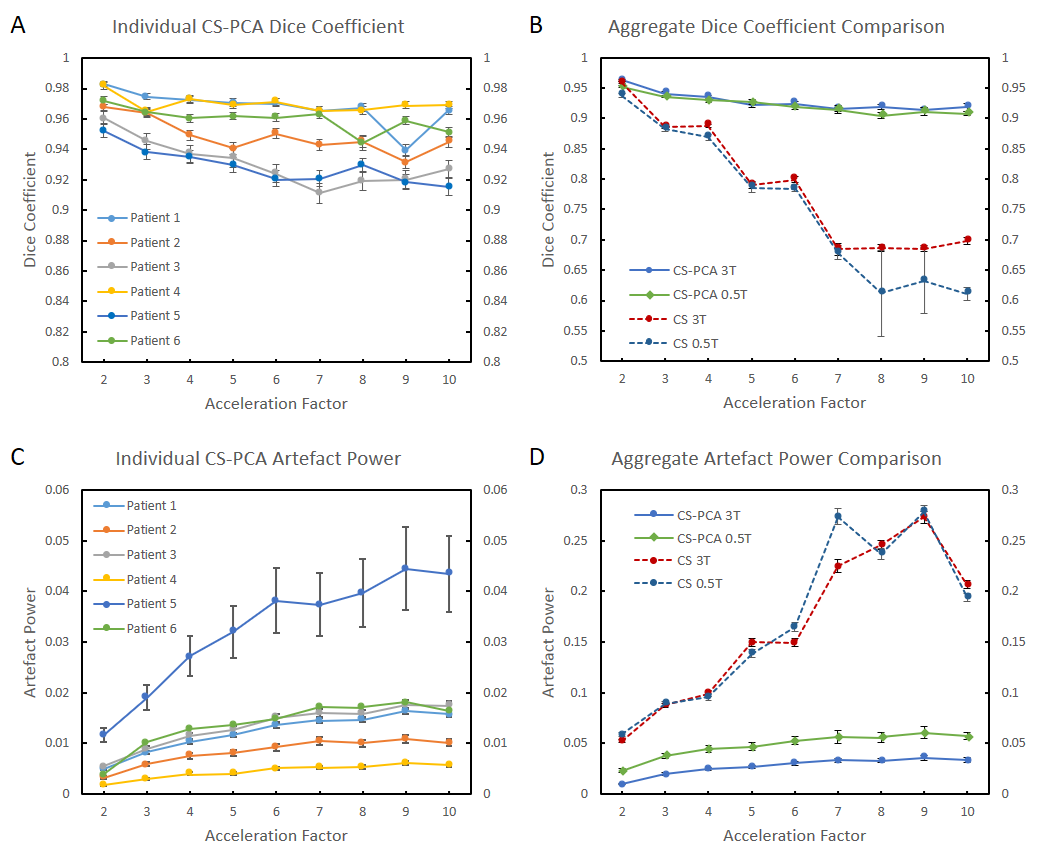
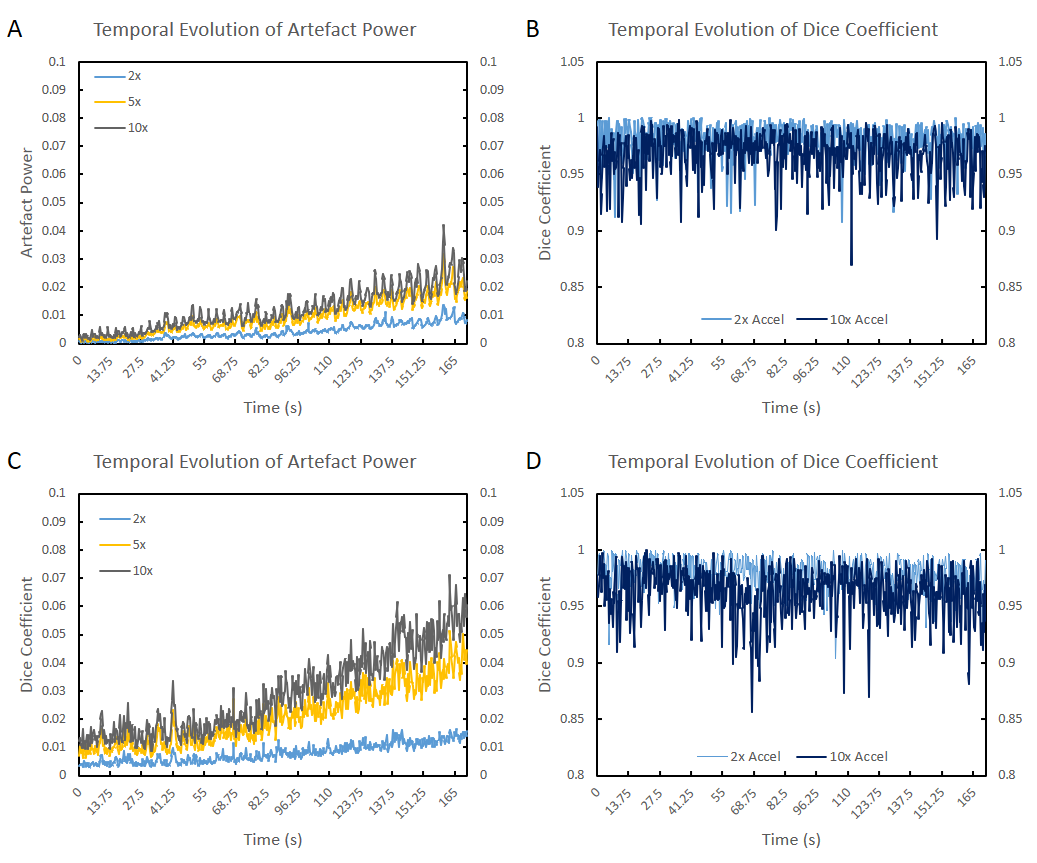
Effective CS-PCA parameters were empirically found to be 10 PCA iterations, a PC threshold ranging from 0.001-0.01, and a database size of 30 images. Figure 3 contains data for the AP and DC for individual patients (A, C), and as a grouped average (B, D). Our results indicate that CS-PCA performed superior than CS alone. Figures 4A and 4C display the temporal evolution of the AP for CS-PCA increased with increasing imaging time; however, as shown in Figure 4B and 4D, the temporal DC remained relatively constant over time (no drifting). Figure 3B reveals that that the patient averaged DC for both 3T and simulated 0.5T data remained above 0.9 for acceleration factors up to 10x. The patient averaged AP (Fig. 3D) gradually increased with increasing acceleration; however, it remained below 0.06 up to an acceleration factor of 10x for both 3T and simulated 0.5T data. The CS-PCA reconstruction speed ranged from 5-20 ms (Intel i7-4710HQ CPU @ 2.5 GHz), depending on the parameters. The reconstruction time was found to be linearly proportional to the database size, such that doubling the database doubles the time. We found that a database size of 30 was sufficient for all patients. Furthermore, the patient averaged AP for the simulated 0.5T data increased for all accelerations; however, the patient average DC did not change from 3T to 0.5T.Conclusion
A real-time reconstruction technique was developed for the purpose of adaptive radiotherapy using our Linac-MR system. Our CS-PCA algorithm can achieve tumour contours with DC greater than 0.9 and AP less than 0.06 at acceleration factors of up to, and including, 10x. The CS-PCA reconstruction speed ranges from 5-20 ms implemented using non-optimized MATLAB code. Further research will investigate the performance of CS-PCA on non-Cartesian data, as well as simultaneous multi-slice and 3D data acquisitions.Acknowledgements
This research was supported by Alberta Innovates Health Solutions (AIHS).References
1. PJ Keall, et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76a. Med. Phys. 2006;33(10):3874-3900.
2. F Zong, M Nogueira, and P Galvosas. Fast reconstruction of highly undersampled MR images using one and two dimensional principal component analysis. MRI. 2016;34:227-237.
3. Goldstein T and Osher S.The Split Bregman Method for L1-Regularized Problems. SIAM. 2009;2(2):323-343.
4. J Yun, E Yip, Z Gabos, K Wachowicz, S Rathee, and BG Fallone. Neural-network based autocontouring algorithm for intrafractional lung-tumour tracking using Linac-MR. Med. Phys. 2015;42(5):2296-2310.
5. E Yip, et al. Prior data assisted compressed sensing: A novel MR imaging strategy for real time tracking of lung tumors. Med. Phys. 2014;41(8):082301 (12pp.).
6. J Yun, et al. Evaluation of a lung tumor autocontouring algorithm for intrafractional tumor tracking using low-field MRI: A phantom study. Med. Phys. 2012;39(3)1481-1494.
Figures