3802
Differential modulation of arterial and venous oxygenation through inhalation of carbogen (95%O2/5%CO2) vs. 100% O2.1Center for Neuroscience and Regenerative Medicine, National Institute of Helath, Bethesda, MD, United States, 2Radiology and imaging sciences, National Institute of Helath, Bethesda, MD, United States
Synopsis
Susceptibility-weighted imaging (SWI) is a MRI sequence which exploits the susceptibility contrast between various tissues by incorporating MRI phase data. In some clinical applications it may be useful to increase such contrast (e.g. identification of plaque associated veins) and in other cases it may be useful to suppress or decrease such contrast (e.g. visualization of microhemorrhage). Here we explore the use of gas inhalation (oxygen and carbogen) to modulate the conspicuity of brain vasculature.
Introduction
Susceptibility-weighted imaging (SWI) is a combination of standard T2*-weighted MRI with image post-processing techniques that enhance the visibility of veins and microhemorrhages by incorporating MRI phase data(1). The contrast in SWI is due to the presence of susceptibility sources such as deoxyhemoglobin in vessels, micro hemorrhages and so on. Segmented 3D EPI sequences allow for highly efficient acquisition of heavily susceptibility weighted images allowing for high resolution visualization of small arteries and veins in relatively short acquisition times (2). For some purposes it may be useful to increase such contrast (e.g. identification of plaque associated veins) and in other cases it may be useful to suppress or decrease such contrast (e.g. visualization of microhemorrhage). Here we explore the use of gas inhalation (oxygen and carbogen) to modulate the conspicuity of brain vasculature.Materials and Methods
MRI acquisition: Three healthy volunteers were scanned on a 3.0 T Biograph mMR (Siemens, release VB20P) after informed consent under an IRB approved protocol. An accelerated 3D segmented EPI protocol was used to acquire high resolution SWI images(2). Imaging parameters used in this study were matrix=340x352x288, voxel size =0.65 mm3, TE/TR = 25 ms/57 ms/12° with ETL = 15. The total scan duration for each acquisition was 4 minutes 45 seconds. SWI images were acquired using a gas inhalation block paradigm. The experimental design used in this study is as described previously (3). The subject is fitted with mouth piece and the mouth piece is connected to the gas bag through a tube. The subject is fitted with mouth piece to allow breathing through the mouth. The composition of gases used in this are oxygen (100% O2) and carbogen (95% O2 + 5% CO2). The subject inhaled room air oxygen as shown in Figure 1 for 10 minutes, followed by 10 minutes of pure oxygen or carbogen, and then followed by another 10 minutes of room air oxygen. Two SWI acquisitions were performed during each block of room air (baseline and recovery) and gas inhalation. Data analysis: The acquired magnitude and phase images were processed using the following steps(4): (1) Laplacian-based phase unwrapping , (2) high pass filtering to remove the background phase, and (3) multiplication of the magnitude and filtered phase to generate enhanced images. For visualization, the SWI images were minimum intensity projected (minIP) over a slab thickness of 25 mm.Results
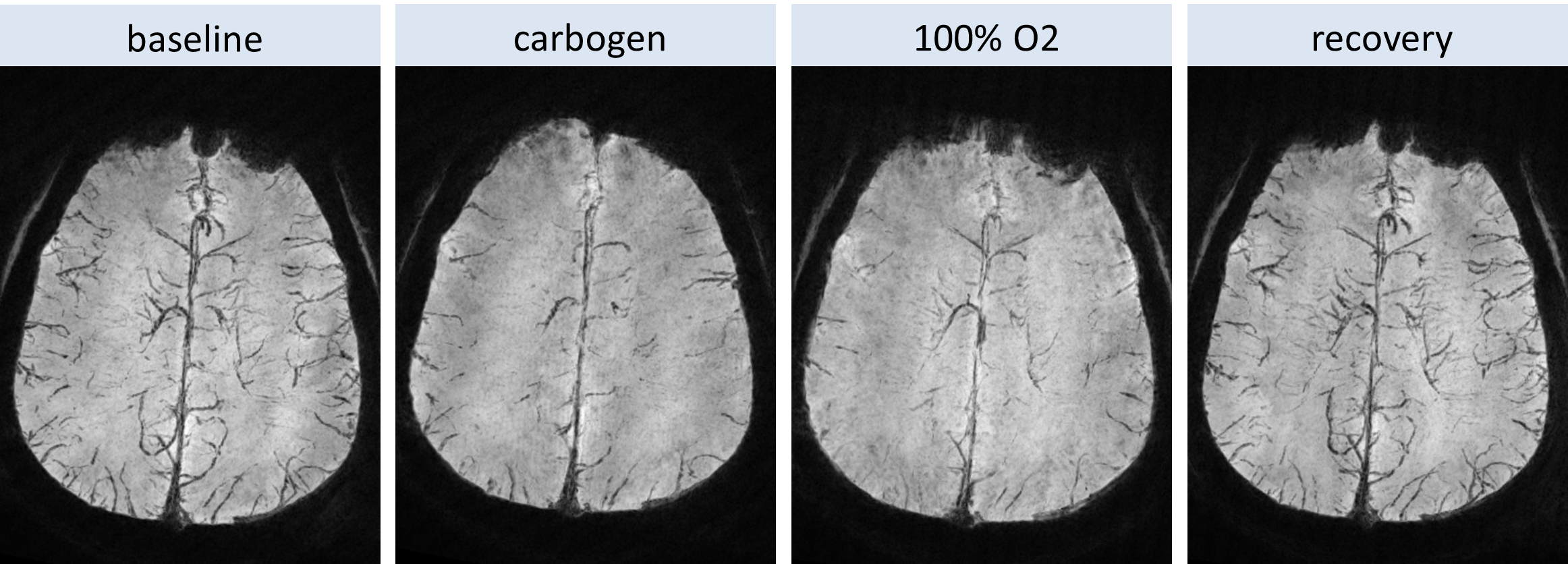
SWI minIP images over 25 mm section thickness are shown (Figure 2). Baseline images show high conspicuity of fine venous structures in the periventricular region and larger veins in the deep venous system. With carbogen, the fine venous structures in the periventricular region virtually completely disappear, and contrast for the deep veins iss considerably reduced. With 100% oxygen, conspicuity of both the smaller and larger venous structures is increased relative to carbogen breathing, but still much less thatn that at baseline. Superficial cortical arteries and veins may be seen at the periphery of the image. Peripheral vessels are less well seen with both carbogen and 100% oxygen. However, in carbogen has relatively lesser effect on the conspicuity of cortical arteries arteries are seen somewhat better with carbogen than with oxygen.Discussion and Conclusion
Inhalation of oxygen and carbogen modulate the conspicuity of cerebral vasculature. The differential effect of carbogen and oxygen on arterial conspicuity can be explained by the physiological response to the respective gases. Regarding the arteries: Inhalation of 100% O2 results in arterial vasoconstriction accounting for the decreased conspicuity of the arteries. The 5%CO2 component of carbogen overrides the arterial vasoconstriction induced by high O2, therefore the arteries are more conspicuous with carbogen than with 100% O2. Regarding the veins: The high o2 content of both gases should increase the O2 saturation of venous blood, resulting in a relative decrease in the fraction of deoxyhemoglobin, and hence less susceptibility induced signal loss. Because veins do not have the ability to vasoconstrict, the more profound effect of carbogen indicates that the veins in the O2 inhalation have lower oxygenation (higher deoxyhemoglobin) than those in the carbogen inhalation. Hyperoxia induced arterial vasoconstrictoin reduces the cerebral blood flow (CBF) relative to carbogen inhalation. With no change in tissue metabolism, a constant oxygen extraction should result in higher venous deoxyhemoglobin concentration as compared with the higher CBF state. CONCLUSION: Inhalation of 100% oxygen vs carbogen both reduce conspicuity of fine vessels seen on high resolution SWI, but affect arteries and veins in a differential manner. We intend to explore whether such modulation can be used to generate clinically useful SWI contrast.Acknowledgements
This work was supported by Center for Neuroscience and Regenerative Medicine (CNRM) and the intramural Program of the National Institutes of Health.References
1. Haacke EM, Mittal S, Wu Z, Neelavalli J, Cheng YC. Susceptibility-weighted imaging: technical aspects and clinical applications, part 1. AJNR American journal of neuroradiology 2009;30:19-30.
2. Sati P, Thomasson DM, Li N, Pham DL, Biassou NM, Reich DS, Butman JA. Rapid, high-resolution, whole-brain, susceptibility-based MRI of multiple sclerosis. Multiple sclerosis 2014;20:1464-1470.
3. Ravi H, Thomas BP, Peng SL, Liu H, Lu H. On the optimization of imaging protocol for the mapping of cerebrovascular reactivity. Journal of magnetic resonance imaging : JMRI 2016;43:661-668.
4. Li N, Wang WT, Sati P, Pham DL, Butman JA. Quantitative assessment of susceptibility-weighted imaging processing methods. Journal of magnetic resonance imaging : JMRI 2014;40:1463-1473.
Figures
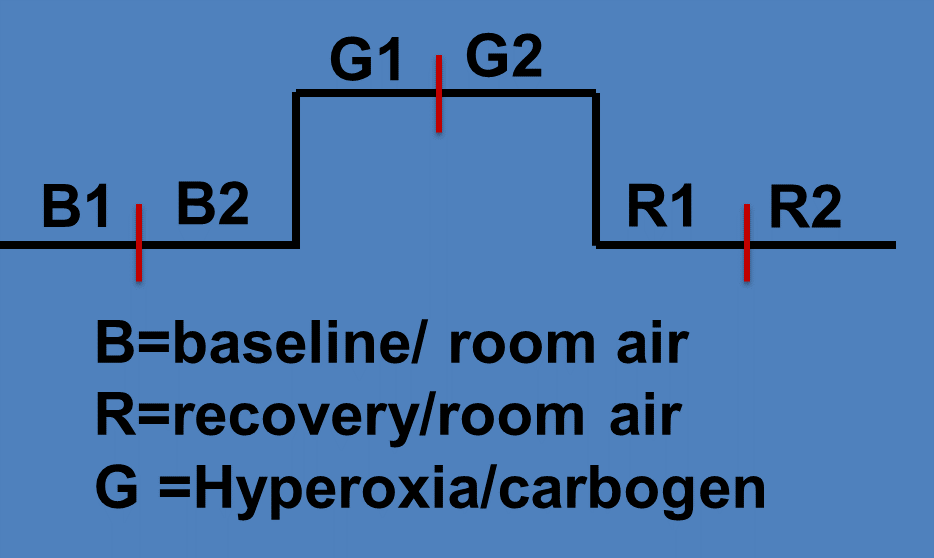
Figure 1: Block paradigm used in this study.