3720
Rapid high-resolution 3D T1 mapping using a highly accelerated radial inversion-recovery FLASH technique1Electrical and Computer Engineering, The University of Arizona, Tucson, AZ, United States, 2Electrical and Computer Engineering, The University of Arizona, 3Biomedical Engineering, The University of Arizona, 4Department of Medical Imaging, The University of Arizona
Synopsis
A golden angle radial IR-FLASH technique and a principle component based iterative algorithm are developed for high-resolution T1 mapping using highly undersampled 3D radial data. The novel method yields T1 maps of a 3D volume with high spatial and temporal resolution and can cover 144 slices within 5 minutes.
Introduction
Quantitative T1 measurements are becoming routine in clinical MRI. To comply with clinical time constraints, various fast T1 mapping techniques have been developed1-5. These methods typically trade-off spatial by temporal resolution to achieve T1 mapping in a reasonable scan time, or are limited to a small number of slices, precluding good slice coverage.In this work we propose a rapid 3D T1 mapping technique based on a golden angle radial inversion-recovery (IR) FLASH acquisition. The technique uses highly undersampled radial data and a model-based reconstruction that enforces temporal sparsity of the T1 recovery curves. The technique enables 3D T1 mapping with high spatial resolution (1mm isotropic) from data acquired with high temporal resolution (25 TI points) within a short scan time.Technique
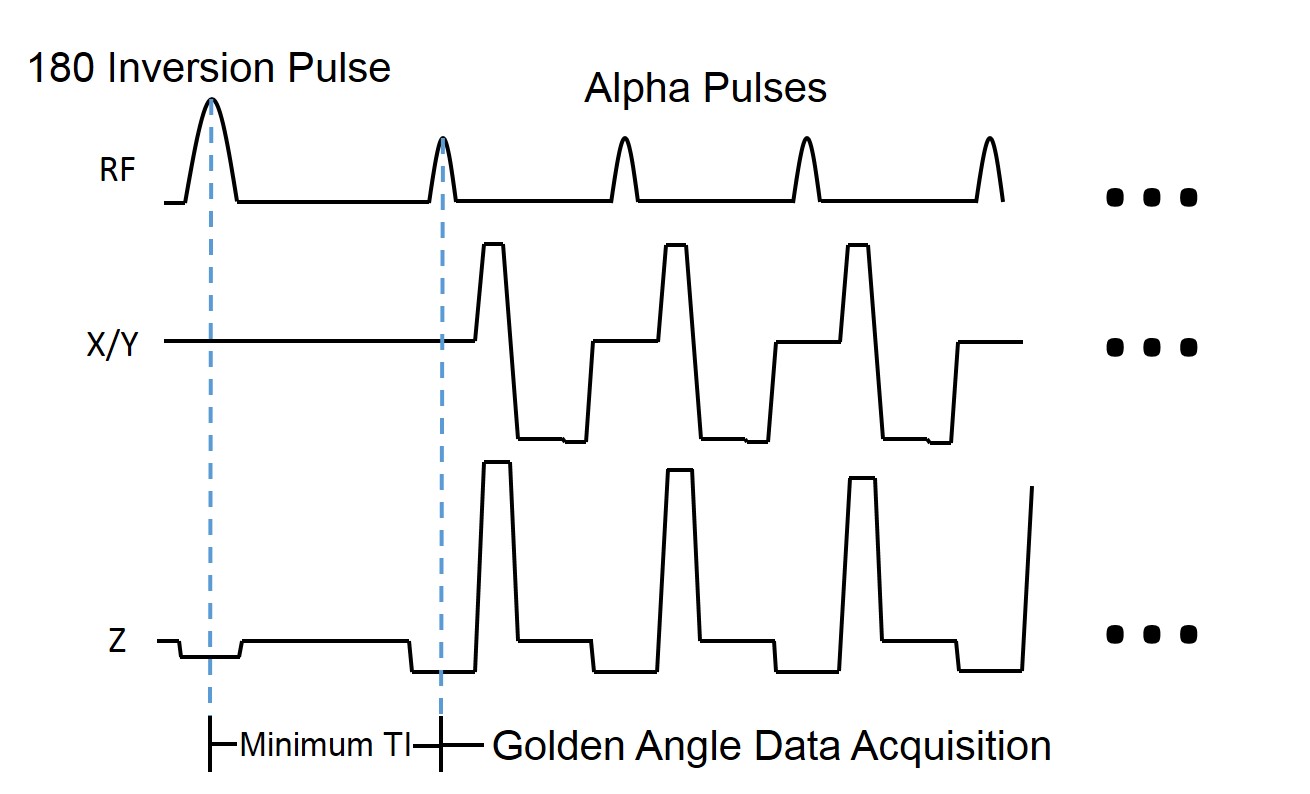
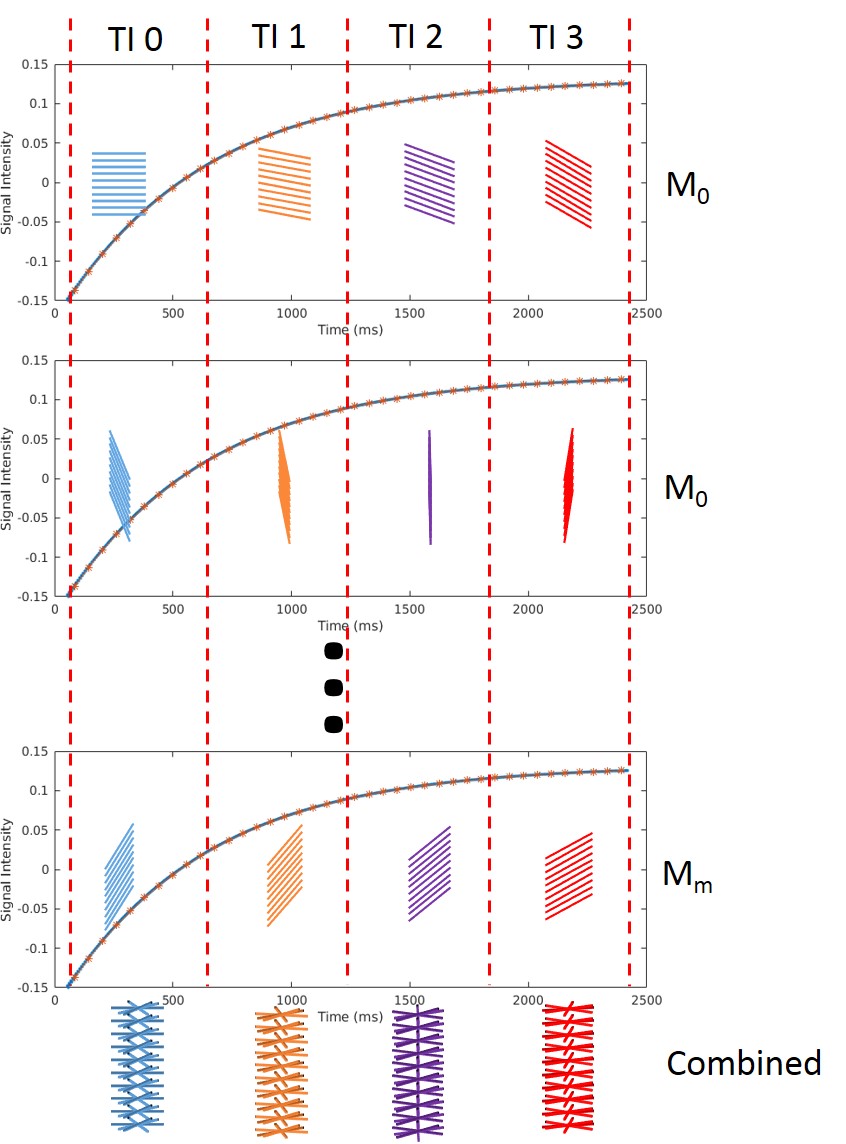
The technique uses a stack-of-stars 3D radial IR-FLASH pulse sequence with golden angle view ordering. As shown in Fig. 1 data for a slab are continuously acquired following a 180o slab-selective inversion pulse. Data acquired after one inversion pulse fills part of the slab’s k-space data needed for T1 mapping, thus, the acquisition is repeated several times (refer here as measurements, M). Figure 2 shows the acquisition order of radial lines. We first collect radial lines at one angle for all kz partitions (as indicated by the blue lines in the figure in M0) and then jump to the next angles (as shown by the orange, purple and red lines) according to an optimized golden angle scheme. After a ~4s collection time, there is a 3s waiting period followed by a second IR-FLASH acquisition to collect radial lines for M1. M measurements are collected to ensure that enough data are acquired for a successful reconstruction.For reconstruction, every P lines collected along kz are considered data for a single TI point, thus N TI points are collected in each measurement, as shown in Fig. 2. The TI time is approximated to the middle TI of this acquisition window. Data from M measurements are combined, ensuring each 3D TI image volume to have M views per partition. To achieve fast imaging each TI data set is highly undersampled (e.g. 3% relative to Nyquist sampling).For T1 mapping an iFFT operation is first used along kz. Since data for each partitions is highly undersampled we use a reconstruction framework based on the inversion-recovery signal model.
$$\hat{T1} = \underset{T1}{\text{argmin}}\sum_{j} ||FT_{j}S_{j} - K_{j}||$$
In Eq. (1) $FT_j$ is the Fourier operator for the jth TI, K_j is the measured k-space data at TIj. S_j is the 3-parameter T1 model proposed in [6], which is a function of T1, TE, TR and flip angle of the excitation RF pulse. The T1 model is linearized using a principal component (PC) basis generated from a set of training curves[5][7-8]. Once the PC coefficients are reconstructed, the TI images are recovered and T1 maps are generated using a method previously described8.Since a slab-selective inversion pulse is used, data from >2 slabs can be acquired in a sequentially by interleaving slabs. This makes the method efficient when high anatomical coverage is needed (e.g. full brain).
Methods
In-vivo data were acquired at 3T. Brain data were acquired with FOV=250mm, matrix size=256x256, TE/TR/alpha=2.27ms/4.30ms/10o with M=12, P=36, N=25 for 4 slabs (33% oversampling). 25 TI imaging volumes (144 slices each) were reconstructed (from 12 radial views per partition) from data acquired in ~4min. Carotid data were acquired using a custom-built neck coil9 with FOV=120mm, matrix size=192x192, TE/TR/alpha=2.85ms/5.40ms/10o, M=16, P=24, N=25, 2 slabs (25% oversampling) in 4min.Results and Discussion
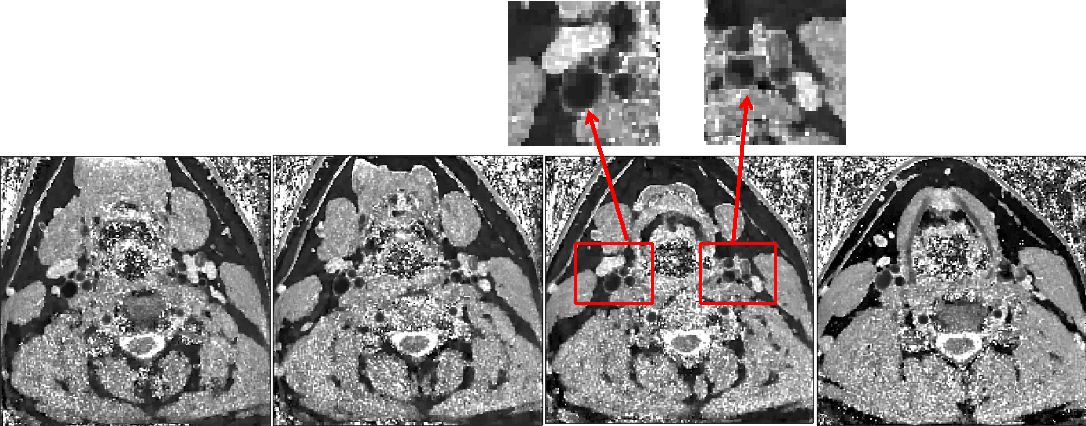
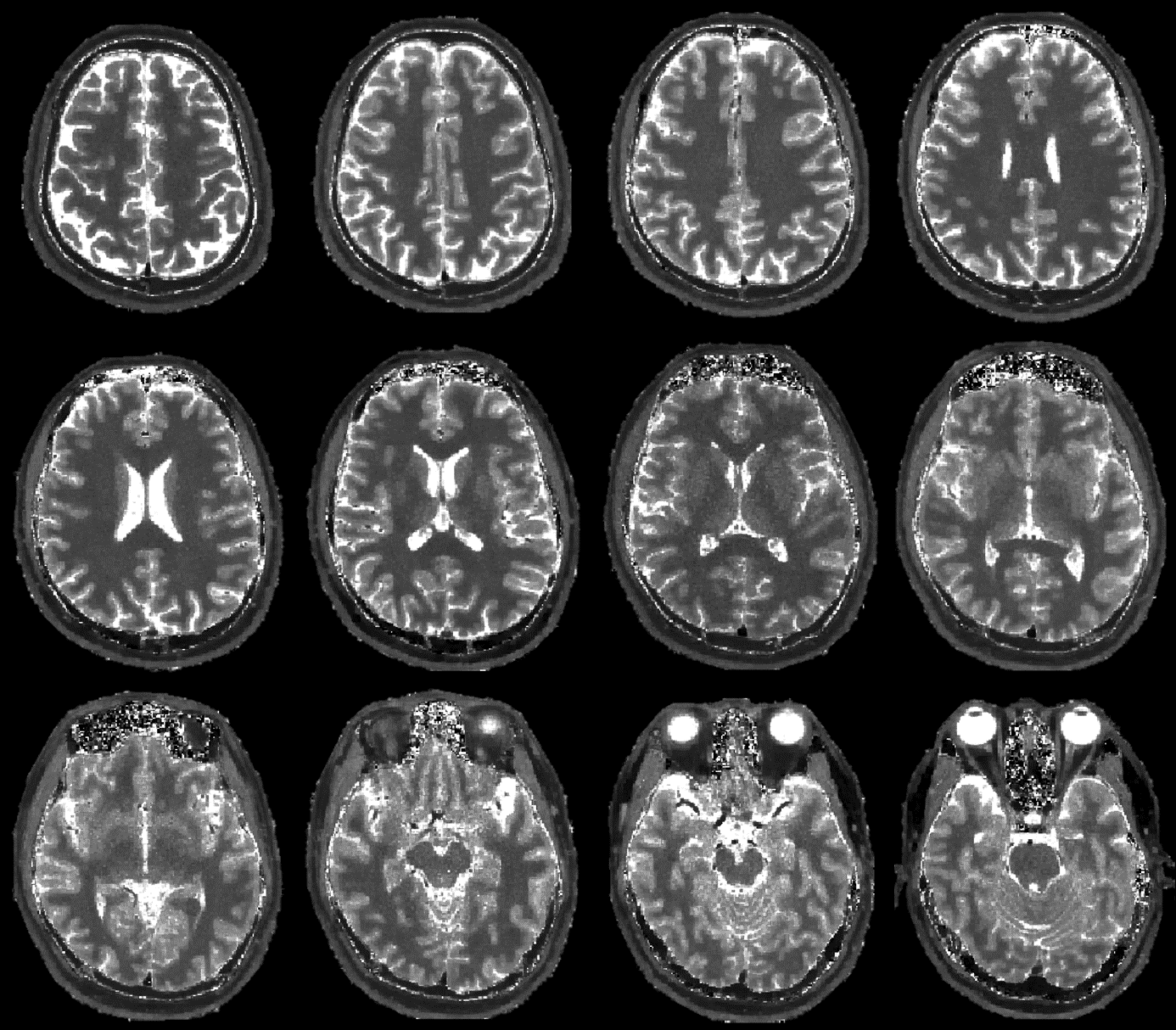
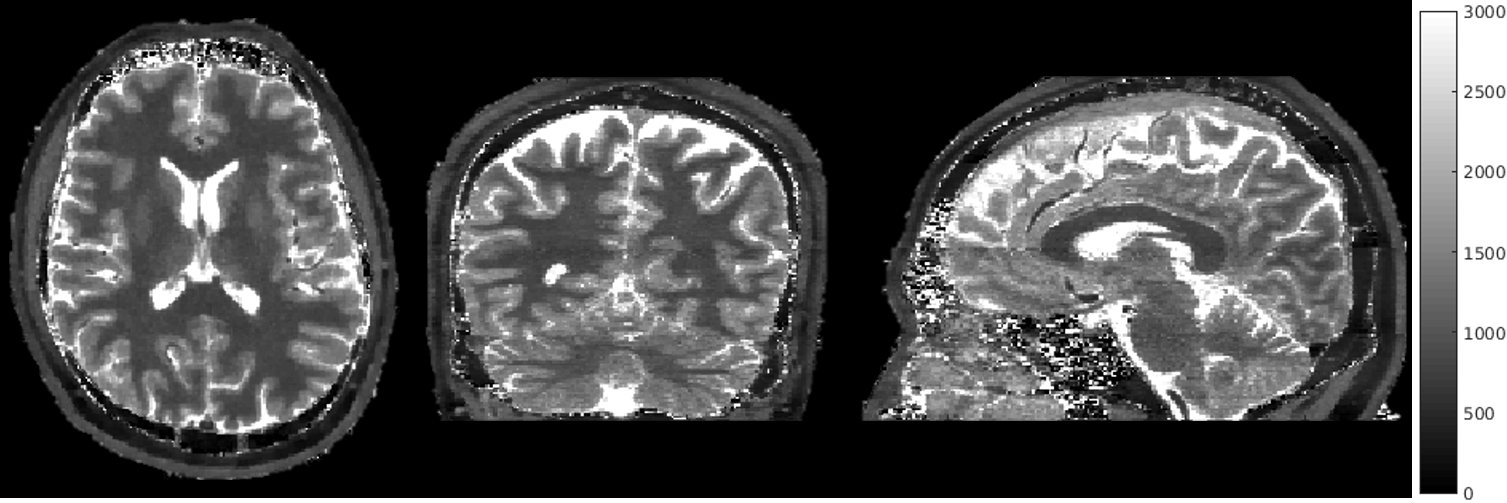
Figure 3 shows 0.64mm x 0.64mm x 1mm T1 maps (4 out of 48 slices) through the neck of a healthy volunteer. Figure 4 shows brain T1 maps (12 out of 144 slices) with 1mm isotropic resolution. Figure 5 shows T1 maps from axial and reformatted sagittal and coronal planes. Note that the spatial details are preserved even with this high level of undersampling. Compared to previous T1 methods that provide comparable spatial resolution1, the acquisition time of the proposed framework is <60%, while providing high temporal resolution (25 TI points) for the T1 fitting, making the results more reliable.Conclusion
We
proposed a fast 3D method for T1 mapping with high spatial and temporal
resolution with scanning times under 5 min. The method should speed up clinical
examinations requiring T1 mapping. Acknowledgements
No acknowledgement found.References
[1] Sean C. L. Deoni, Terry M. Peters and Brian K. Rutt, High-Resolution T1 and T2 Mapping of the Brain in a Clinically Acceptable Time with DESPOT1 and DESPTO2, Magn Reson Med 2005; 53: 237-241.
[2] Dan Ma, Vikas Gulani, Nicole Seiberlich, Kecheng Liu, Jeffrey L. Sunshine, Jeffrey L. Duerk and Mark A. Griswold, Magnetic Resonance Fingerprinting, Nature 2013; 495: 187-192.
[3] Mariya Doneva, Peter Börnert, Holger Eggers, Christian Stehning, Julien Sénégas and Alfred Mertins, Compressed Sensing Reconstruction for Magnetic Resonance Parameter Mapping, Magn Reson Med 2010; 64: 1114-1120.
[4] Barral JK, Gudmundson R, Stikov N, Etezadi-Amoli M, Stoica P, Nishimura DG, A robust methodology for in vivo T1 mapping, Magn Reson Med 2010, 64:1057-1067.
[5] Zhitao Li, Benjamin P. Berman, Jean-Philippe Galons, et al. Rapid high-resolution T1 mapping using highly accelerated radial steady-state free-precession acquisition. ISMRM 2016.
[6] R. Deichmann, A. Haase, Quantification of T1 Values by SNAPSHOT-FLASH NMR Imaging, JMR 1992; 96(3): 608-612.
[7] Chuan Huang, Christian G. Graff, Eric W. Clarkson, Ali Bilgin, and Maria I. Altbach, T2 mapping from highly undersampled data by reconstruction of principal component coefficient maps using compressed sensing. Magn Reson Med 2012; 67: 1355-1366.
[8] Chuan Huang, Ali Bilgin, Tomoe Barr and Maria I. Altbach, T2 Relaxometry with Indirect Echo Compensation from Highly Undersampled Data. Magn Reson Med 2012; 70: 1026-1037.
[9] Michael Beck, Dennis Parker, Bradley Bolster Jr., Seong-Eun Kim, J McNally, Gerald Treiman, J, Hadley, Interchangeable Patient-Specific Receive-Only Carotid Coils for Simultaneous Imaging with Radio Frequency Head Coils at 3 Tesla, ISMRM 2016.
Figures