3566
Pancreatic exocrine function estimated by cine dynamic MRCP with a spatially selective IR pulse: Correlation with T1 mapping of the pancreatic parenchymaKatsuyoshi Ito1, Akira Yamamoto1, Kazuya Yasokawa1, Minoru Hayashida1, Daigo Tanimoto1, Akihiko Kanki1, Tomohiro Sato1, Hidemitsu Sotozono1, Takeshi Fukunaga1, Koji Yoshida1, Kazunori Moriya1, and Tomoyuki Okuaki2
1Radiology, Kawasaki Medical School, Kurashiki, Japan, 2Philips Healthcare AsiaPacific, Japan
Synopsis
This study assessed the correlation between pancreatic exocrine function estimated by cine dynamic MRCP with a spatially selective IR pulse and T1 mapping of the pancreatic parenchyma on 3T MR imaging. There was a statistically significant correlation between the secretion grade of the pancreatic juice in cine-dynamic MRCP and T1 relaxation time of the pancreatic parenchyma. Therefore, T1 mapping of the pancreatic parenchyma will be used as collaborative, noninvasive technique of cine-dynamic MRCP with a spatially selective IR pulse for the estimation of pancreatic exocrine function.
Purpose
To assess the correlation between pancreatic exocrine function estimated by cine dynamic MRCP with a spatially selective IR pulse and T1 mapping of the pancreatic parenchyma on 3T MR imaging.Materials and Methods
Twenty-five patients with suspected hepatobiliary and pancreatic diseases underwent abdominal MR imaging including cine dynamic MRCP with a spatially selective IR pulse and T1 mapping of the pancreatic parenchyma on 3T MRI. In cine dynamic MRCP imaging, a spatially selective IR pulse (inversion time; 2200 msec) was placed on the pancreatic head perpendicular to the main pancreatic duct with width of 20 mm. This pulse was used to null the signal from the static pancreatic juice (Fig.1). When the pancreatic juice is secreted and flows in the pancreatic duct, inflow of the pancreatic juice is observed as a high signal within the area of IR pulse (Fig.2). MRCP using a spatially selective IR pulse was repeatedly performed every 15 seconds (4-seconds scan and 11-seconds rest) during a period of 5 minutes (a total of 20 single-shot images). A set of these 20 consecutive MRCP images obtained repeatedly at single level was termed as cine dynamic MRCP with a spatially selective IR pulse. Cine dynamic MRCP images were evaluated for the secretion grade of the pancreatic juice, which was categorized according to the distance that the pancreatic juice moved in the pancreatic duct within the area with a spatially selective IR pulse using the following 5-point secretion grading scale (grade 0, no secretion; grade 1, ≤5 mm; grade 2, 6–10 mm; grade 3, 11–15 mm; grade 4, >15 mm). The secretion grade of cine dynamic MRCP images in each patient was defined as follows: (total of grading score in 20 images)/20. Quantitative T1 relaxation time maps were derived automatically on a voxel-by-voxel basis. The MR data sets were transferred to a workstation to measure the T1 relaxation time of the pancreatic parenchyma using operator-defined regions of interest (ROIs). Special attention was given to drawing ROI circles in a homogenous region of the parenchyma avoiding volume averaging from retroperitoneal fat, vessels, and pancreatic duct. Additionally, the signal intensities of the pancreatic parenchyma (SIp) and paraspinal muscle (SIm) on fat-suppressed T1-weighted gradient echo images were measured for calculation of the signal intensity ratio (SIR=SIp/SIm).Results
The mean T1 relaxation time of the pancreatic parenchyma measured from T1 mapping was 978.6 +/- 285.8 msec (range: 594 – 1845 msec) while the mean secretion grade of the pancreatic juice in cine-dynamic MRCP with a spatially selective IR pulse was 1.02 +/- 0.92 (range: 0 – 2.75). There was a statistically significant correlation between the secretion grade of the pancreatic juice in cine-dynamic MRCP and T1 relaxation time of the pancreatic parenchyma (p=0.002) (Fig.3). In 13 patients with secretion grade less than 0.70 in cine-dynamic MRCP which can be used a cutoff value for the criterion of pancreatic exocrine insufficiency, the mean T1 relaxation time (1107.2 +/- 342.6 msec) was significantly higher than that (839.3 +/- 97.6 msec) in 12 patients with normal pancreatic exocrine function (p=0.017) (Figs.4,5). SIR tended to correlate with T1 relaxation time of the pancreatic parenchyma and secretion grade in cine-dynamic MRCP, but the difference was not statistically significant (p=0.09, 0.08, respectively).Conclusion
T1 mapping of the pancreatic parenchyma will be used as collaborative, noninvasive technique of cine-dynamic MRCP with a spatially selective IR pulse for the estimation of pancreatic exocrine function.Acknowledgements
No acknowledgement found.References
No reference found.Figures
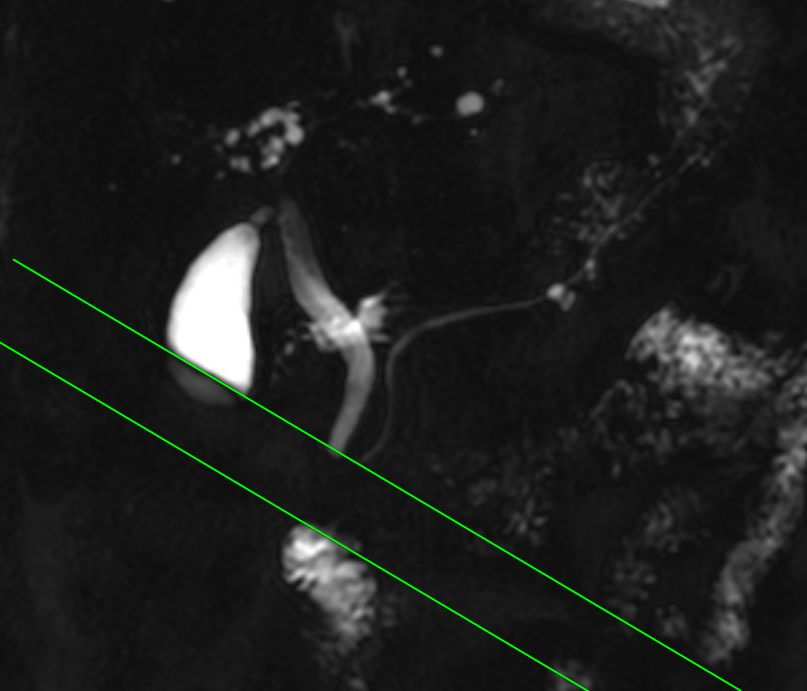
Cine dynamic MRCP with a spatially selective IR pulse. Secretion grade=0 (no flow within the area of IR pulse).
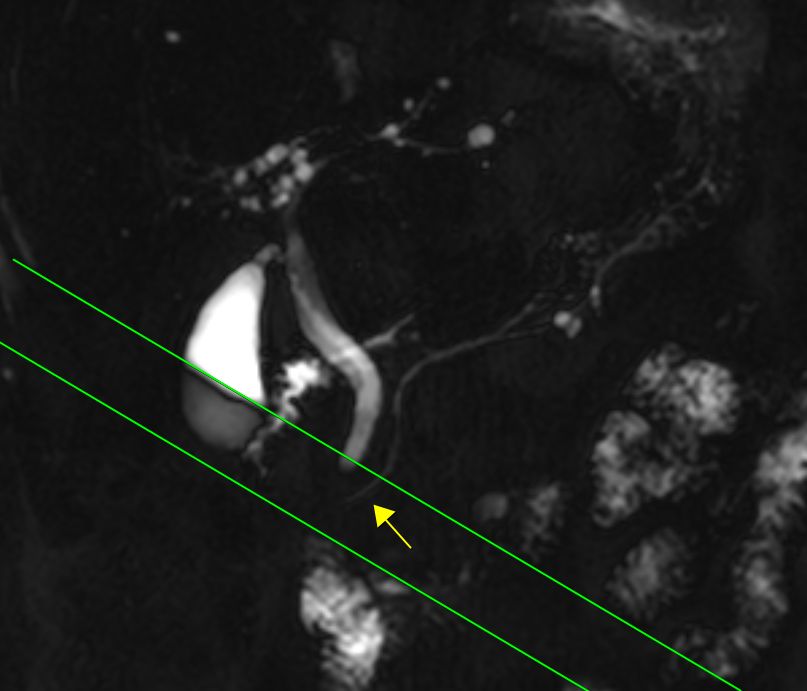
Cine dynamic MRCP with a spatially selective IR
pulse. Secretion grade=2 (10mm inflow with high signal within the area of IR
pulse).
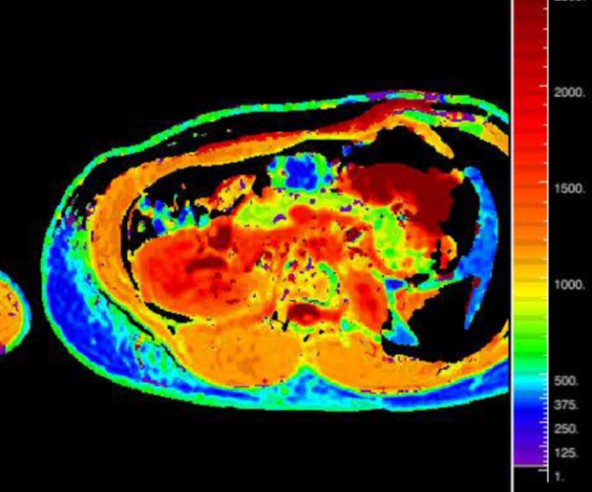
T1 map image in a patient with normal pancreatic exocrine function. T1 relaxation time of pancreatic parenchyma was 819 msec.
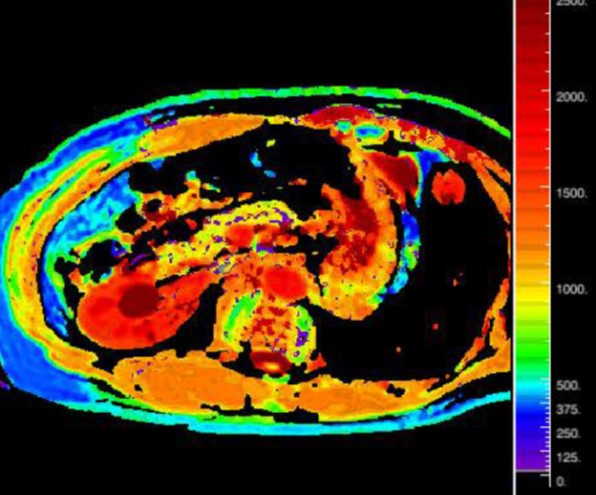
T1 map image in a patient with mild pancreatic exocrine insufficiency. T1 relaxation time of pancreatic parenchyma was 1023 msec.
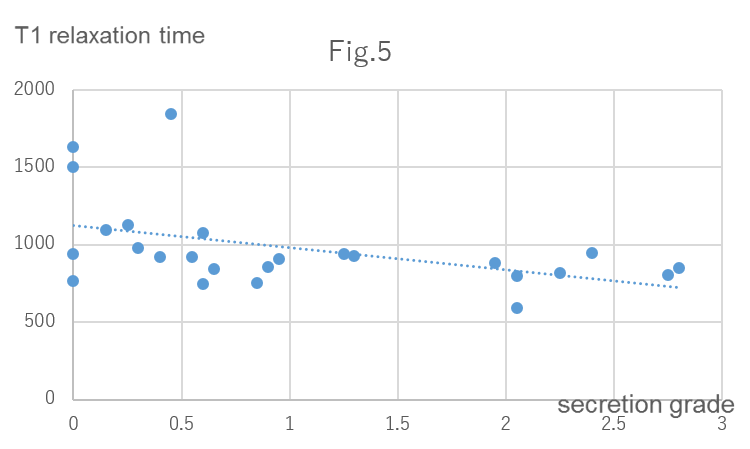
Correlation between T1 relaxation time of the pancreatic parenchyma measured from T1 mapping and the mean secretion
grade in cine-dynamic MRCP with a spatially selective
IR pulse.