3563
Qualitative and Quantitative Comparison of 2D Gradient Recalled Echo and Rapid 2D Gradient Recalled Echo Magnetic Resonance Elastography1UCLA, Los Angeles, CA, United States, 2Siemens Healthcare, United States
Synopsis
Conventional GRE-based MR elastography requires a breath hold of approximately 18 seconds per slice, which is difficult for some patients. We compared a rapid GRE-based sequence (9 second breath hold) to conventional GRE in terms of quantitative liver stiffness (LS) measurement and image quality score (IQS), based on wave propagation and confidence mask coverage, determined by two independent radiologists. The two sequences were equivalent in terms of LS measurement, but the rapid GRE sequence had significantly higher IQS for both readers. Rapid GRE-based MR elastography may be an improved alternative to GRE in patients with limited breath hold capacity.
Introduction
Because of its ability to estimate stiffness in large sections of the liver, hepatic magnetic resonance elastography (MRE) is quickly becoming the standard for non-invasive assessment of liver fibrosis.1 The standard clinical implementation available from multiple vendors is a gradient-recalled echo (GRE) based phase contrast technique, which acquires each line of k-space twice with the polarity of the motion encoding gradient (MEG) reversed. With the 60 Hz oscillating external mechanical frequency applied in standard clinical tests, a TR of 50 ms (3 mechanical cycles) is typically used to acquire these two measurements at the same mechanical phase while accommodating the 16.7 ms MEG. Using parallel imaging to acquire the four necessary phase offsets this requires a breath hold of around 18 sec for the elasticity measurement on each slice. This breath hold time can be halved using rapid GRE MRE, which leverages the periodicity of the applied mechanical motion and subtracts two measurements acquired with the same MEG polarity but timed so that the mechanical motion is 180 degrees out of phase.2 This methodology allows the use of a 25 ms TR (1.5 mechanical cycles). With the same k-space sampling, this results in a 9 sec breath hold per slice. Given that the standard clinical protocol calls for a breath hold at end expiration, the shorter breath hold duration is important to accommodate the clinical patients for which the longer breath hold in conventional GRE MRE may be difficult.Purpose
To compare 2-dimensional (2D) GRE and 2D rapid GRE MRE sequences in the liver in terms of quantitative liver stiffness (LS) measurement and image quality.Methods
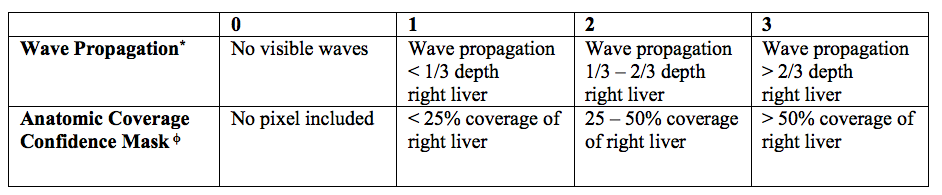
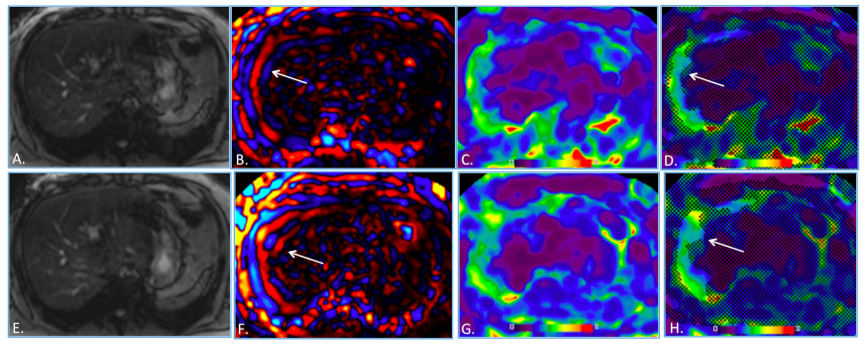
This IRB-approved, HIPAA-compliant, prospective study involved 27 consecutive subjects (14 men, 13 women; mean age 52 years, range 21 – 75 years) who underwent liver MRI at 3.0 T (MAGNETOM Prisma, Siemens Healthcare, Erlangen Germany), including two different MRE sequences during the same session, 2D GRE (TR, 50 msec; TE, 22 msec; slice thickness, 5 mm; gap, 1 mm; matrix, 77 x 128; flip angle, 250; breath hold, 18 sec) and 2D rapid GRE prototype (TR, 25 msec; TE, 22 msec; slice thickness 5 mm; gap, 1 mm; matrix, 84 x 128; flip angle, 150, breath hold, 9 sec). Image quality scores (IQS) were evaluated by two independent observers based on wave propagation and right hepatic lobe coverage on the confidence mask (0-15), based on a previously published technique.3 This technique is described in Figure 1. One of the two observers measured LS on stiffness maps (in kilopascal, kPa) for each sequence. Mean LS, region of interest sizes (based on confidence mask) and image quality scores were compared using paired nonparametric Wilcoxon test. Inter-reader reliability for IQS was assessed using Cohen’s kappa.Results
LS measurements were not significantly different between the two sequences (2.65 + 0.98 kPa for GRE vs 2.54 + 1.04 kPa for rapid GRE, P = 0.49). ROI size was not significantly different between the two sequences (13497 + 7338 mm2 for GRE vs 15244 + 6831 mm2 for rapid GRE, P = 0.24). IQS were significantly higher for rapid GRE compared to GRE for both readers (11.6 + 3.3 vs 9.9 + 4.4, P < 0.02, Reader 1; 11.7 + 3.4 vs 9.9 + 4.4, P < 0.02, Reader 2). Inter-reliability was good to very good (κ 0.63 – 0.82).Conclusion
Rapid GRE may be an improved alternative to GRE, especially in patients with limited breath hold capacity. LS measurements are equivalent among the two sequences, but IQS are superior for rapid GRE.Acknowledgements
No acknowledgement found.References
1. Venkatesh SK, Yin M, Ehman RL. Magnetic resonance elastography of liver: technique, analysis, and clinical applications. J Magn Reson Imaging. 2013;37(3):544-55.
2. Chamarthi SK, Raterman B, Mazumder R, et al. Rapid acquisition technique for MR elastography of the liver. Magn Reson Imaging. 2014;32(6):679-83.
3. Wagner M, Besa C, Bou Ayache J, et al. Magnetic resonance elastography of the liver: qualitative and quantitative comparison of gradient echo and spin echo echoplanar imaging sequences. Invest Radiol 2016;51(9):575-81.
Figures