3561
Steatohepatitic Hepatocellular Carcinoma: Distinctive MR Imaging Features with Pathologic and OPTN Correlation1Radiology, Mayo Clinic Arizona, Phoenix, AZ, United States, 2Pathology, Mayo Clinic Arizona, Phoenix, AZ, United States
Synopsis
Hepatocellular carcinoma (HCC) has specific imaging criteria such as arterial hyperenhancement, contrast washout, and pseudocapsule that allow it to be diagnosed with confidence and relative accuracy. However, a novel HCC variant, steatohepatitic hepatocellular carcinoma (SH-HCC), has been described which tends to not exhibit the classic HCC imaging features. In this study, we explored alternative secondary MR features of HCC such as T1 and T2 signal intensity, intralesional fat, and restricted diffusion which may be more applicable in diagnosing steatohepatitic hepatocellular carcinoma.
Introduction
Hepatocellular carcinoma (HCC) is one of the most prevalent tumors worldwide and a leading cause of cancer-related deaths.1 In contradistinction to other major solid organ malignancies, HCC is primarily diagnosed by its imaging features alone. As such, the organ procurement and transplant network (OPTN)/united network for organ sharing (UNOS) has established specific radiologic criteria for HCC classification.2 However, a novel subtype associated with non-alcoholic fatty liver disease (NAFLD)/non-alcoholic steatohepatitis (NASH) and metabolic syndrome has been pathologically described, steatohepatitic hepatocellular carcinoma (SH-HCC),3 which frequently does not exhibit the currently specified appearance for HCC. Although the prevalence of the SH-HCC variant has been reported in the pathology literature as between 14-19% (19 cases in a study of 101 explant livers4 and 16 cases of 118 explant livers3), to our knowledge, this is the first study describing the unique imaging features of SH-HCC based on its pathologic presentation.Methods
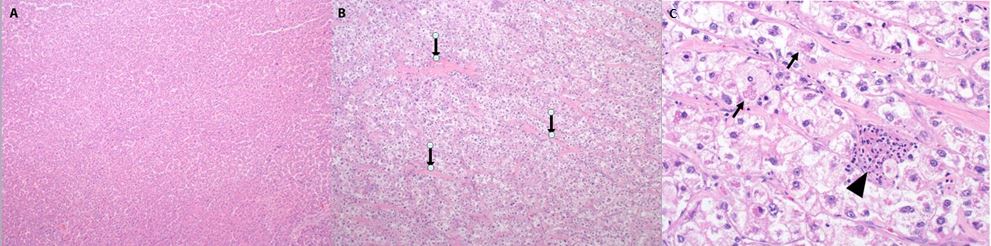
A retrospective search of the Mayo Clinic pathology database from 2011-2016 identified 42 steatohepatitic hepatocellular carcinoma tumors in 23 patients (Fig 1). Two radiologists in consensus (2 and 16 years’ experience) reviewed the abdominal MR obtained just prior to transplantation or resection for each patient. The T1w in- and opposed-phase; T2w; multiphase post-contrast (precontrast, arterial, portal venous; delay); and diffusion weighted sequences were reviewed for OPTN-defined imaging features of HCC (arterial hyperenhancement; washout; pseudocapsule) as well as secondary MR characteristics which favor HCC (T2w hyperintensity; intralesional fat, restricted diffusion). Preoperative OPTN classification was determined from the original radiology reports, excluding those from outside institutions. Patients without preoperative MR imaging and lesions <1.0 cm were also excluded.Results
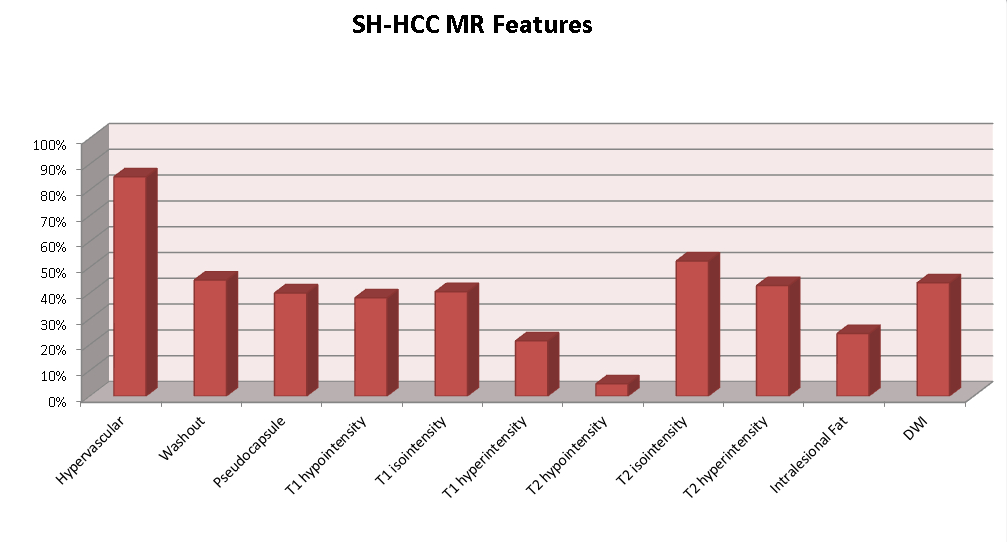
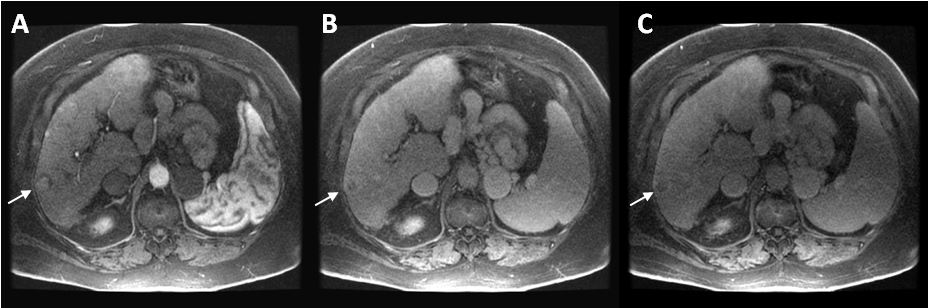
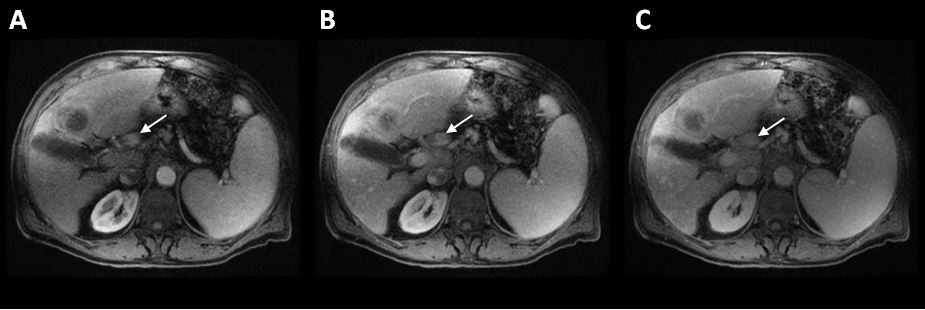
14% (6/42) of SH-HCC were not visualized on MR imaging prospectively, while 12% (5/42) lesions were not visualized retrospectively. In the tumors demonstrable on imaging (Fig 2), individual classic HCC MR features observed: arterial enhancement 34/40 (85%)/washout 18/40 (45%)/pseudocapsule 16/44 (40%). T1 intensity distribution was 16/42 (38%) hypointense, 17/42 (40%) isointense, and 9/42 (21%) hyperintense. T2 intensity distribution was 2/42 (5%) hypointense, 22/42 (52%) isointense, and 18/42 (43%) hyperintense. Other features include presence of intralesional fat 5/26 (19%) and restricted diffusion 18/40 (45%) with 4/40 (10%) positive on both low and high b-values. Preoperative OPTN classification of demonstrable lesions was OPTN 5 (Fig 3) 10/36 (28%) and OPTN 4 or less (Fig 4) 20/36 (56%). Retrospective OPTN classification of tumors on imaging studies was OPTN 5 14/40 (35%) and OPTN 4 or less 20/40 (50%). In the tumors that were 1-2cm in size, 4/24 (17%) was categorized as OPTN 5, and 20/24 (83%) were categorized as OPTN 4 or less, including fully imperceptible tumors. In the tumors >2cm in size, 6/12 (50%) were OPTN 5 and 6/12 (50%) were OPTN 4 or less.Discussion
This study suggests that current HCC imaging guidelines have low sensitivity for SH-HCC, with only 28% of the demonstrable tumors meeting OPTN 5 criteria, and another 14% imperceptible prospectively on imaging. Retrospectively, the percentage of tumors identified as OPTN 5 increased to 38%, however, 62% of the pathology proven SH-HCC tumors were either not visible or displayed at most OPTN 4 characteristics. This is even more problematic for the smaller (1-2cm) tumors, as 83% could not be categorized as OPTN 5. As such, more scrutiny and careful surveillance of OPTN 4 masses is warranted, particularly in the setting of NAFLD/NASH or metabolic syndrome.Conclusion
Steatohepatitic hepatocellular carcinoma is a novel variant that frequently does not display classic imaging features of HCC. Thus, familiarity and increased understanding of their imaging patterns would facilitate better identification of these lesions. Future investigations may require advanced quantitative and functional imaging techniques to improve tissue characterization for improved SH-HCC diagnosis.Acknowledgements
No acknowledgement found.References
1. Ferlay J, Shin HR, Bray F et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-2917.
2. Rosenkrantz AB, Campbell C, Wehrli N, et al. New OPTN/UNOS Classification System for Nodules in Cirrhotic Livers Detected with MR. Radiology 2015;275(2):426-433.
3. Salomao M, Remotti H, Vaughan R, et al. The steatohepatitic variant of hepatocellular carcinoma and its association with underlying steatohepatitis. Hum Pathol. 2012;43:737-746.
4. Jain D, Nayak NC, Kumaran V, et al. Steatohepatitic Hepatocellular carcinoma, a morphologic indicator of associated metabolic risk factors: A study from India. Arch Pathol Lab Med. 2013;137:961-966.
Figures