3550
MR Imaging Characteristics of Benign and Malignant Biliary Strictures1Department of Radiology and Imaging Sciences, Emory University School of Medicine, Atlanta, GA, United States
Synopsis
Wide spectrum of hepatobiliary and pancreatic diseases can lead to development of benign and malignant biliary strictures such as cholangiocarcinoma, pancreatic adenocarcinoma, ampullary carcinoma, PSC, autoimmune pancreatitis, ischemic strictures, post cholecystectomy, trauma etc. MRI characteristic of malignant strictures such as length, location, wall thickness, asymmetry, luminal regularity and enhancement will be discussed. CE_MRI helps to reach specific diagnosis and narrow differential diagnosis which is important for management and treatment planning
Learning Goals:
1. To determine various causes of benign and malignant biliary strictures and their MRI characteristics.
2. Role of combined CE-MRI and MRCP in the evaluation of bile ducts in patients with obstructive jaundice
3. Demonstrate important elements in the assessment and management of benign and malignant biliary strictures.
Background Information and Content:
The purpose of this exhibit is to describe imaging characteristics of combined contrast enhanced MRI and MRCP to differentiate malignant from benign biliary strictures along with histopathological findings such as cholangiocarcinoma, pancreatic adenocarcinoma, IgG4 cholangiopathy, ischemic strictures etc. CE-MRI and MRCP is a noninvasive method in evaluation of patients with obstructive jaundice without ionizing radiation to reach definite diagnosis ERCP with tissue biopsy or surgery is needed for definite diagnosis of biliary strictures but certain MR imaging characteristics are helpful in narrowing the differential diagnosis. Various causes of bile duct strictures and other characteristics are important for diagnosis and management.Key Anatomic, Pathophysiologic Issues, Imaging Findings and Imaging Technique:
A wide spectrum of hepatobiliary and pancreatic diseases can lead to development of benign and malignant biliary strictures such as cholangiocarcinoma, pancreatic adenocarcinoma, ampullary carcinoma, PSC, autoimmune pancreatitis, ischemic strictures, post cholecystectomy, trauma etc. The purpose of this education poster is to describe imaging characteristics of combined contrast enhanced MRI and MRCP to differentiate malignant from benign biliary strictures along with histopathological findings. CE-MRI and MRCP is a noninvasive method in evaluation of patients with obstructive jaundice without ionizing radiation to reach definite diagnosis but ERCP with tissue biopsy or surgery is needed for definite diagnosis of biliary strictures but certain MR imaging characteristics are helpful in narrowing the differential diagnosis such as such as length, location, wall thickness, asymmetry, luminal regularity and enhancement.. MRI protocol and advantages over other modalities will be discussed in addition to treatment planning and management.Conclusions:
1. Combined CE-MRI and MRCP play a key role in characterization of benign and malignant biliary stricture such as CCA, pancreatic adenocarcinoma, PSC, autoimmune pancreatitis, AIDS etc.
2. MRI helps to reach specific diagnosis and narrow differential diagnosis which is of utmost importance for management and treatment planning
Acknowledgements
No acknowledgement found.References
1.Worawattanakul S, Semelka RC, Noone TC, Calvo BF, Kelekis NL, Woosley JT (1998) Cholangiocarcinoma: spectrum of appearances on MR images using currenttechniques. Magnetic resonance imaging 16 (9):993-1003
2. Jarnagin WR (2000) Cholangiocarcinoma of the extrahepatic bile ducts. Seminars in surgical oncology 19 (2):156-176
3. Yamaguchi K, Enjoji M (1987) Carcinoma of the ampulla of vater. A clinicopathologic study and pathologic staging of 109 cases of carcinoma and 5 cases ofadenoma. Cancer 59 (3):506-515
4. Kim JH, Kim MJ, Chung JJ, Lee WJ, Yoo HS, Lee JT (2002) Differential diagnosis of periampullary carcinomas at MR imaging. Radiographics : a review publicationof the Radiological Society of North America, Inc 22 (6):1335-1352. doi:10.1148/rg.226025060
5. Semelka RC, Kelekis NL, John G, Ascher SM, Burdeny D, Siegelman ES (1997) Ampullary carcinoma: demonstration by current MR techniques. Journal ofmagnetic resonance imaging : JMRI 7 (1):153-156
6.LaRusso NF, Shneider BL, Black D, Gores GJ, James SP, Doo E, Hoofnagle JH (2006) Primary sclerosing cholangitis: summary of a workshop. Hepatology(Baltimore, Md) 44 (3):746-764.
7. Kawaguchi K, Koike M, Tsuruta K, Okamoto A, Tabata I, Fujita N (1991) Lymphoplasmacytic sclerosing pancreatitis with cholangitis: a variant of primarysclerosing cholangitis extensively involving pancreas. Human pathology 22 (4):387-395
8. Girometti R, Brondani G, Cereser L, Como G, Del Pin M, Bazzocchi M, Zuiani C (2010) Post-cholecystectomy syndrome: spectrum of biliary findings at magneticresonance cholangiopancreatography. The British journal of radiology 83 (988):351-361. doi:10.1259/bjr/99865290
9. Keleman AM, Imagawa DK, Findeiss L, Hanna MH, Tan VH, Katz MH, Goodwin SC, Lane JS, Vajgrt D, Nguyen T, Smith CW (2011) Associated vascular injury inpatients
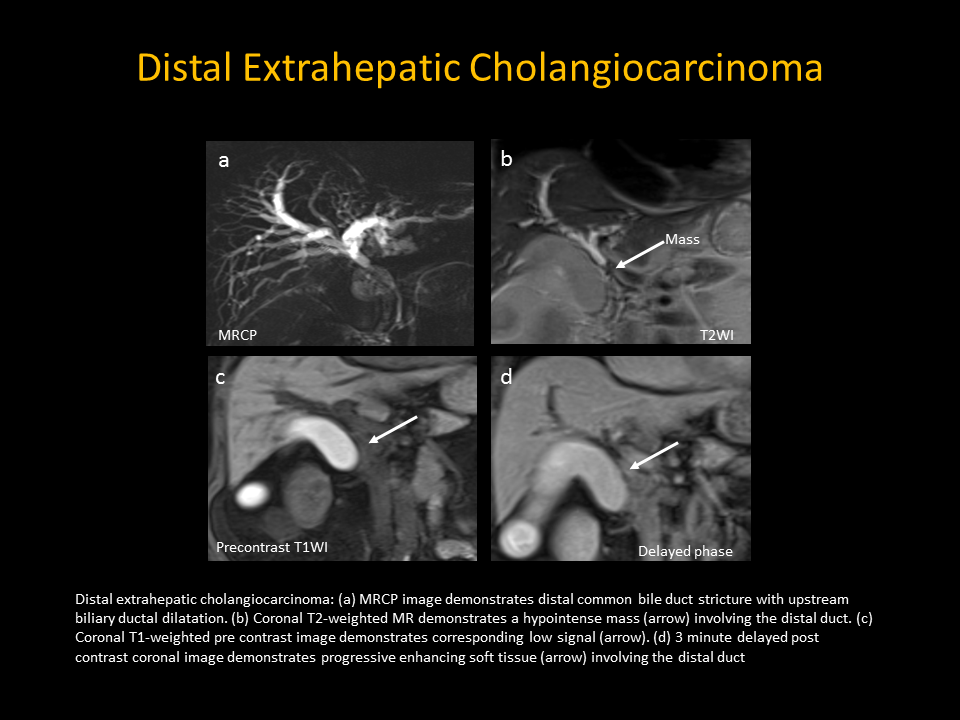
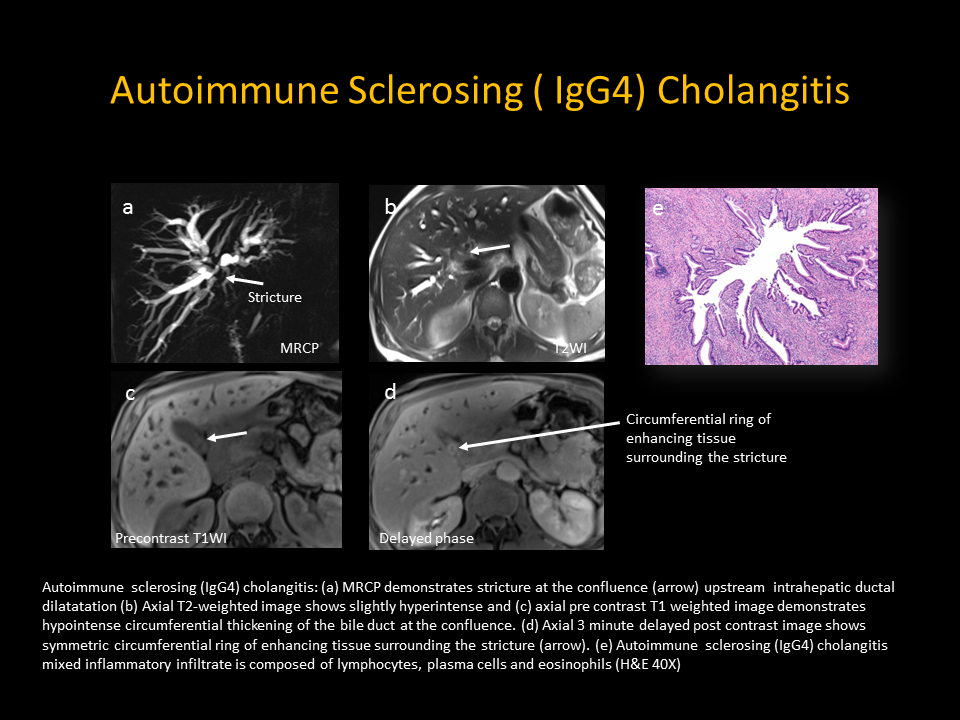
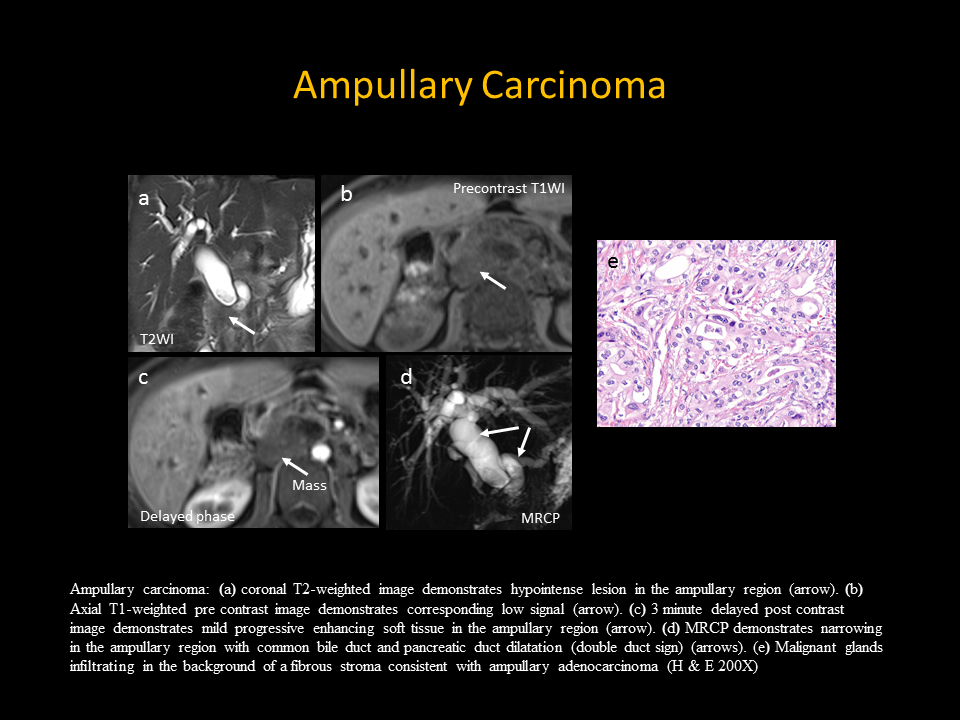
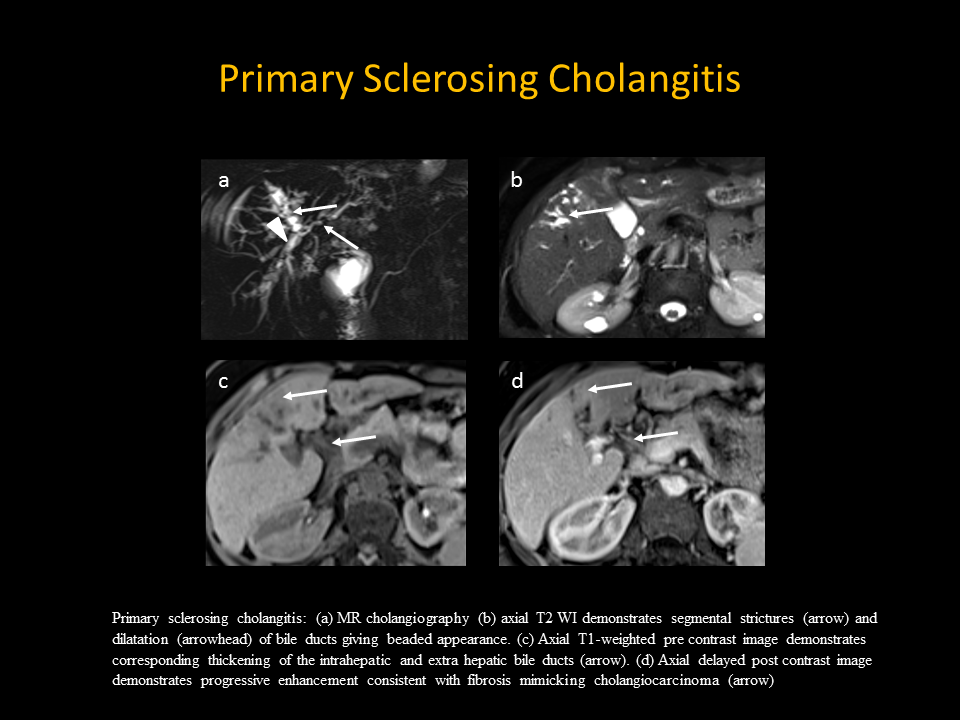
Figures