3546
4D-MRI with 3D radial sampling and self-gating-based K-space sorting: image quality improvement by slab-selective excitation1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3Radiation Oncology, Cedars-Sinai Medical Center, 4Siemens Healthcare R&D, Chicago, IL, United States, 5Siemens Healthcare R&D, Los Angeles, CA, United States, 6Medicine, University of California, Los Angeles, Los Angeles, United States
Synopsis
Stereotactic body radiation therapy with a simultaneous integrated boost (SBRT-SIB) has been used to improve tumor resection rate by sterilizing cancerous tissue that are surrounding the vessels. Accurate tumor imaging and tumor motion assessment will enhance the potential for SBRT-SIB. 4D-MRI (respiratory resolved, 3D volumetric images) has emerged as a promising imaging technique for characterizing tumor motion due to the absence of ionizing radiation and its superior soft tissue contrast. This study explored a slab-selective excitation approach to increase the blood vessel to tissue contrast with the goal of improving the accuracy of boost volume definition in radiation therapy.
Purpose
Pancreatic ductal adenocarcinoma (PDA) is a disease with dismal outcome and high morbidity. The main treatment modality is surgery, however, the primary tumor associated with PDA often surrounds/encases the nearby vasculature, thereby making the tumor unresectable in most cases. Stereotactic body radiation therapy (SBRT) with simultaneously integrated boost (SIB) has been used to improve tumor resection rate by sterilizing tissues surrounding the vessels. Accurate tumor imaging and tumor motion assessment would enhance the design of SBRT-SIB. Due to the absence of ionizing radiation and the superior soft tissue contrast, four-dimensional magnetic resonance imaging (4D-MRI) has emerged as a promising imaging technique for characterizing tumor motion in the abdomen. Recently, a novel 4D-MRI technique using 3D radial sampling and self-gating based k-space sorting was proposed to characterize abdominal respiratory motion1. This study aimed to improve the technique by using slab-selective (SS) excitation to increase vessel-tissue contrast and reduce streaking artifacts. The improvements from the SS approach on image quality was investigated through comparisons with non-selective excitation (NS) with clinical 4D computed tomography (CT).Method
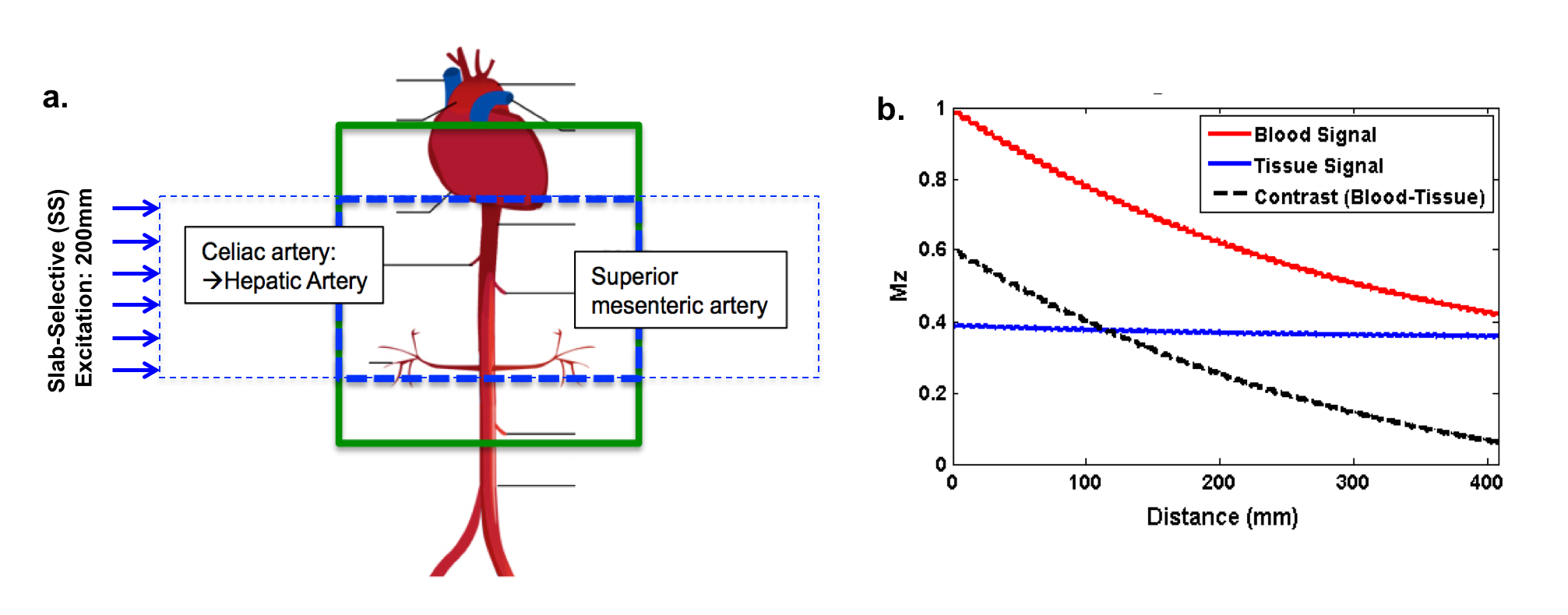
MR sequence: A spoiled gradient recalled echo prototype sequence with 3D radial k-space sampling was used for data acquisition. 1D projection based self-gating was used for respiratory motion detection and golden-angle k-space trajectory was used to enable arbitrary k-space sorting. A slab-selective (SS) excitation was used where approximately half of the superior-inferior volume covering the region of interest was excited compared to that in the previously proposed non-selective (NS) excitation approach (Figure 1a).
Theory: Figure 1b shows the simulation of blood and tissue longitudinal magnetization (signal) and their contrast versus their distance. The target tissue repeatedly sees the RF pulses and reaches a steady-state. Fresh blood flowing into the imaging volume has not experienced any RF pulses, thus exhibiting maximum signal at the entrance. Vessel-tissue contrast is therefore preserved as the blood experiences less RF pulses than static tissues when traversing the imaging volume.
Experiment: Two excitation approaches, SS and NS 4D-MRI, were compared in 7 cancer patients (1 liver and 6 pancreatic cancer) and 2 healthy subjects at 3T (Biograph mMR, Siemens Healthcare, Germany). Vessel-tissue contrast ratio (CR), contrast-to-noise ratio (CNR), and signal-to-noise ratio (SNR) were assessed in all subjects. Vessel-tissue contrast of NS and SS 4D-MRI and 4D-CT were also compared in six of the pancreatic patients. No contrast was administered for 4D-MRI. Residual contrast from previous CT scans was present during 4D-CT. CR was defined as the difference between blood vessel (large: aorta; small: superior mesenteric artery or vein) signal near the center of the field-of-view (FOV) and its nearby tissue. CNR was defined as the ratio of CR and standard deviation (SD) of a region of interest (ROI) of nearby air. SNR was measured as the ratio of the signal of the blood vessel of interest to the SD of ROI of air. Image artifact was assessed in consensus in 6 of the subjects by two reviewers on a 4-point scale (0: poor; 3: excellent) to evaluate the advantage of SS in reducing image artifacts. Imaging parameter: FOV = (400 mm)3; prescribed spatial resolution = (1.56 mm)3; FA = 12o; TR/TE = 110.60/ 2.68 ms; readout bandwidth = 429 Hz/pixel; 10 respiratory bins.
Results
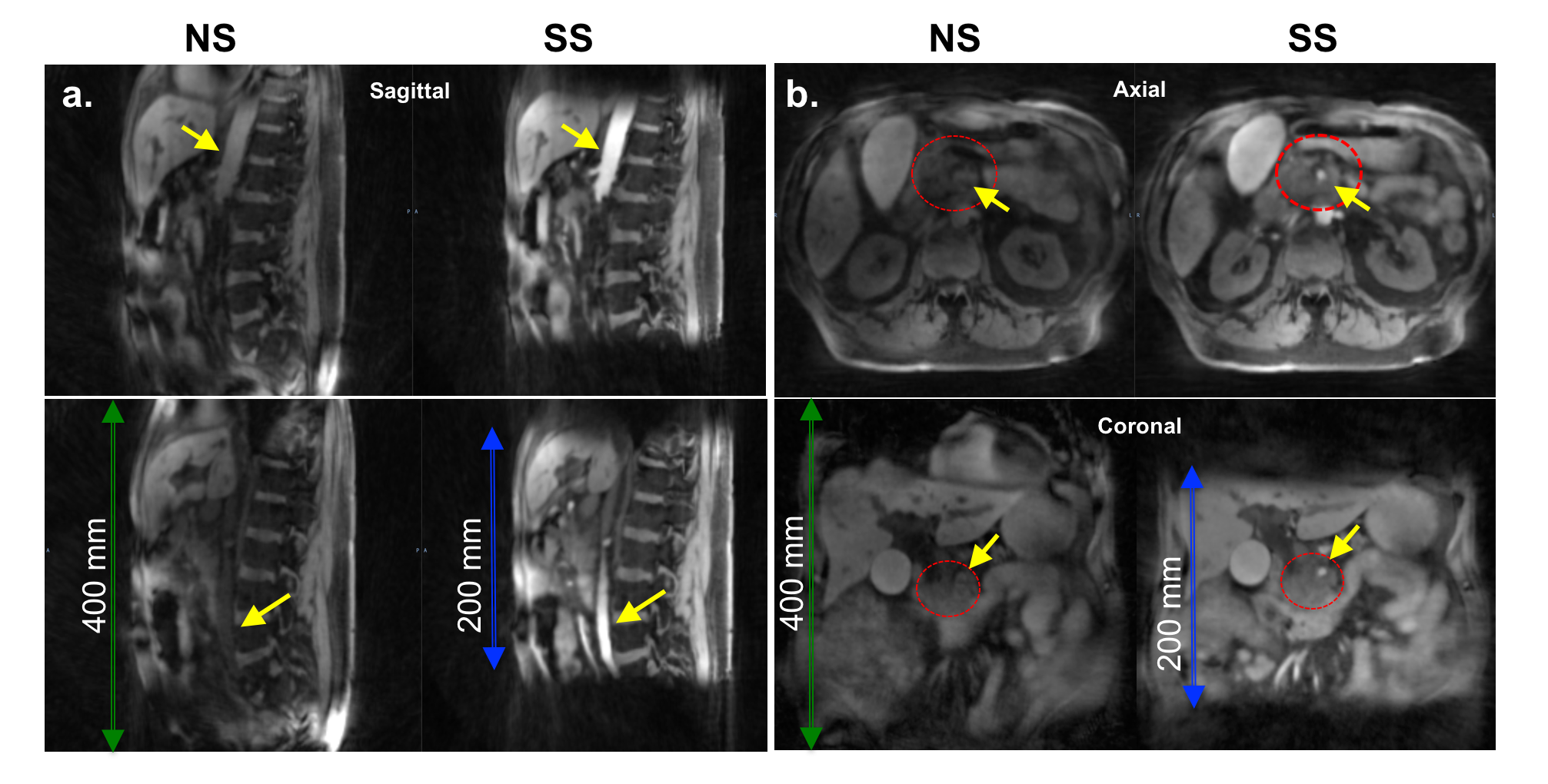
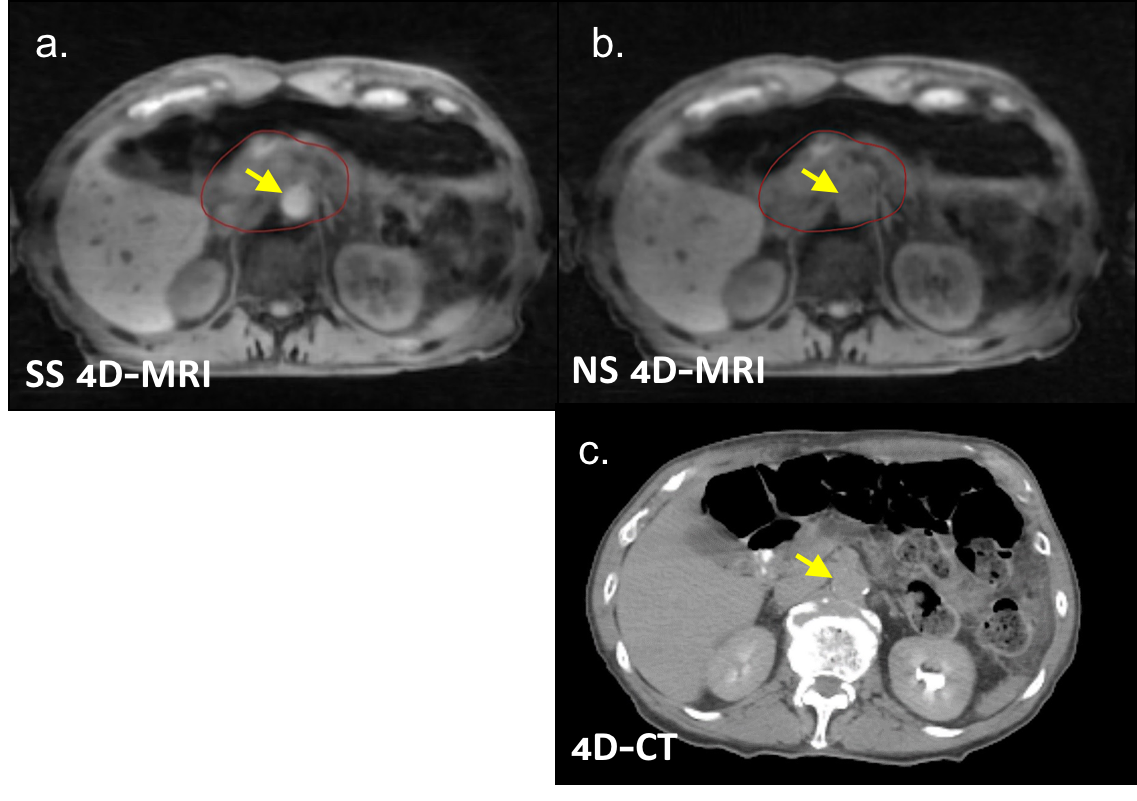
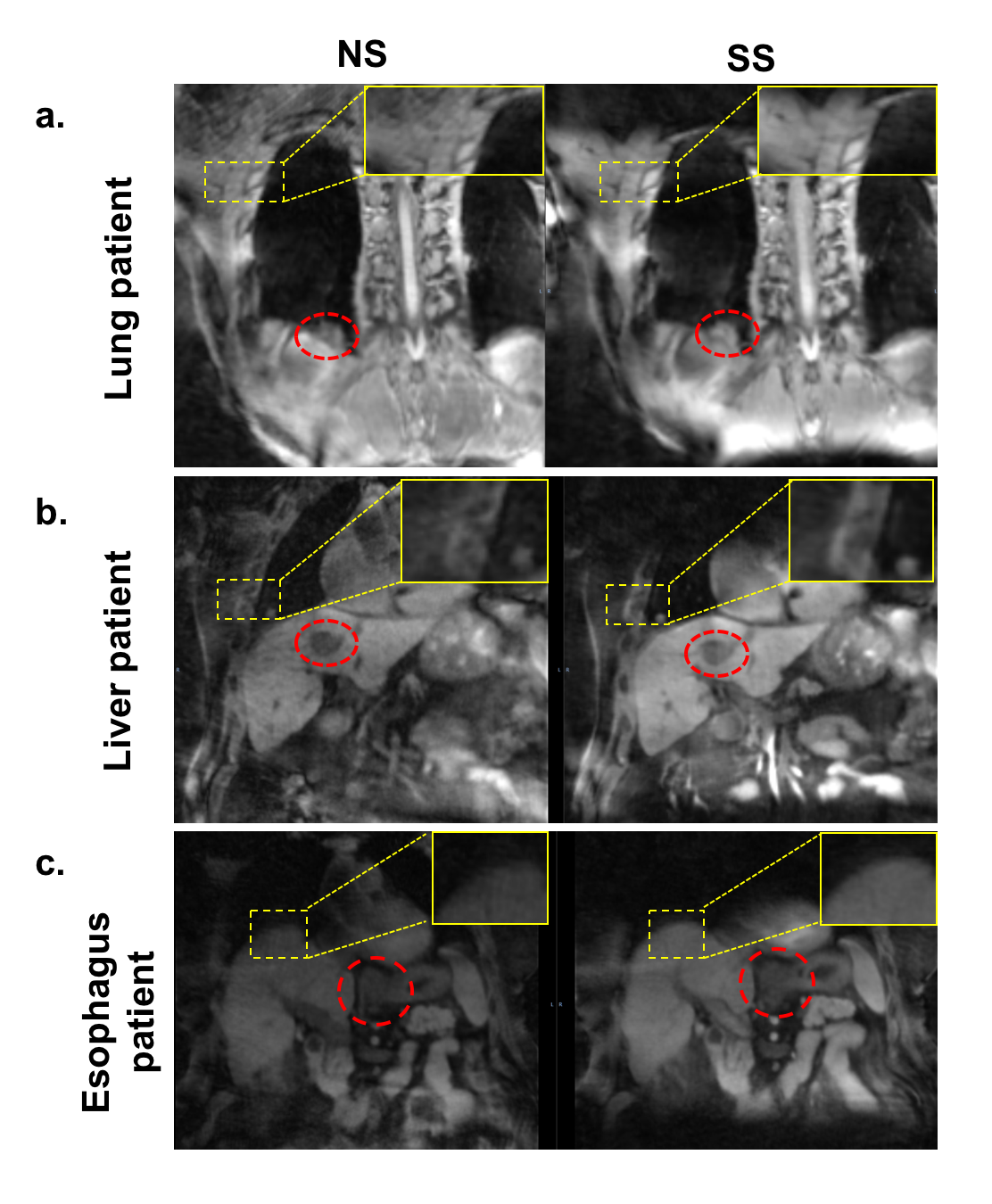
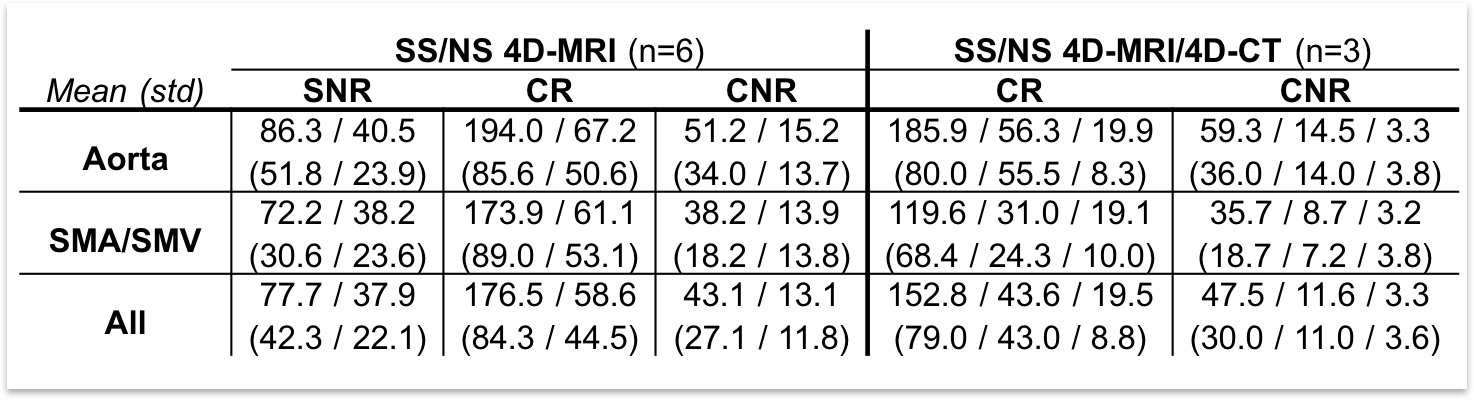
Compared with NS 4D-MRI (n=9), SS 4D-MRI images had significantly overall higher CR (176.5±84.3 vs. 58.6±44.5, p<0.001), CNR (43.1±27.1 vs. 13.1±11.8, p<0.001), and SNR (77.7±42.3 vs. 37.9±22.1, p<0.001) by >2-folds increase. Compared with 4D-CT (n=6), NS 4D-MRI images had slightly higher CR (43.6±43.0 vs. 19.5±8.8, p=0.07) and CNR (11.6±11.0 vs. 3.3±3.6, p=0.05), whereas SS 4D-MRI images had significantly higher CR (152.8±79.0 vs. 19.5±8.8, p<0.001) and CNR (47.5±30.0 vs. 3.3±3.6, p<0.001) by >7-fold increase. When looking at the large and small vessels individually, similar results were observed and summarized in Table 1. Figure 2 shows an example illustrating the improvement in vessel-tissue contrast in both large and small vessels when using NS compared to SS methods. Among NS 4D-MRI, SS 4D-MRI, and 4D-CT, SS 4D-MRI provided the best delineation at the interface between tumors and infiltrated vessels as shown in Figure 3. In addition, image quality was visually improved by SS versus NS (2.7±0.5 vs. 1.5±0.5), mainly due to markedly reduced streaking artifacts in lung, liver, and esophagus cases (Figure 4).Conclusion
The proposed 3D radial sampling with slab-selective excitation improved vessel-tissue CR and CNR, blood SNR, and overall image quality when comparing with non-selective excitation and 4D-CT. SS 4D-MRI showed great potential in accurate definition of boost volumes for pancreatic radiation therapy which may enhance the design of SBRT-SIB for PDA.Acknowledgements
No acknowledgement found.References
1. Deng et al. Four-dimensional MRI using three-dimensional radial sampling with respiratory self-gating to characterize temporal phase-resolved respiratory motion in the abdomen. Magn Reson Med. 2016 Apr;75(4):1574-85.Figures