3490
High Resolution Facial Nerve Tractography in Patient with Vestibular Schwannoma1Center for Brain Imaging Science and Technology, Department of Biomedical Engineering, Zhejiang University, Hangzhou, People's Republic of China, 2Department of Neurosurgery, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, People's Republic of China, 3Application Team, Siemens Healthcare, Shanghai, People's Republic of China
Synopsis
Reliable tractography of specific abnormal brain nerves such as the facial nerve displaced by vestibular schwannoma is necessary for estimating risk before the surgery. Single-shot diffusion EPI sequence has been used previously to reconstruct tractography of facial nerve but suffered severe distortion in the basicranial region. Here we performed high resolution anatomical and diffusion scans in patients with vestibular schwannoma, in order to track the facial nerve and provide reliable result for the surgeons to evaluate the surgical risk.
Purpose
Vestibular schwannoma is a common intracranial tumor deriving from vestibular nerve. The development of microneurosurgical techniques and intraoperative neurophysiological monitoring increases the surgery success rate of the total tumor resection and the facial and vestibulocochlear nerve preservation. However, surgeons need to estimate the orientation of the displaced facial nerve before surgery in order to preserve its function. Diffusion tractography can potentially illustrate specific nerve orientation and tumor morphology before the operation and help the surgeons to design an appropriate process for each patient.1-5 Previous studies 1-4 used single-shot diffusion EPI sequences to track the facial nerve located in the basicranial region where distortions usually occurs, and the misregistration between the diffusion and anatomy images often mislead selecting proper seed ROIs and consequently the correct tracking.
In this work, high resolution anatomical images using ZOOMit excitation and less distorted diffusion images using the Read-out Segmentation Of Long Variable Echo-trains (RESOLVE) were obtained to improve tractography outcomes in facial nerves.
Methods
The scans were performed on a 3T scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a 64 channel head coil. High resolution anatomy images were acquired using the T2-weighted 3D Turbo Spin Echo sequence with ZOOMit excitation (TR/TE=1000/128 ms, FOV=160x82x28 mm, voxel size=0.5 mm isotropic, turbo factor=80, echo spacing=7.36 ms, bandwidth=256 Hz/Px, average=3.5) for better visualization for drawing the seed ROI. Less distorted diffusion images were acquired using the RESOLVE (TR/TE=3000/48 ms, FOV=230x130 mm, voxel size=1.8 mm isotropic, slice number=20, iPAT=2, segments=9, echo spacing=0.34 ms, b-value=800 mm2/s, diffusion directions=20 at hemisphere) for better co-registration with the structural images. The total scan time was 20 minutes which was well tolerated by the patients.
Diffusion tensor tractography was then performed in the multimodality workstation employing the deterministic tracking algorithm by using the fourth order Runge-Kutta method. The seed ROI was selected in the region of the cerebellopontine angle cistern in the interpolated 3D anatomical space of the T2 images. Two samples per voxel with a step size of 0.3 mm was used in the tracking process. The stopping criteria included FA threshold of 0.18, and the angle threshold of 40 degree.
The operation of resecting the vestibular schwannoma from the patient was performed in the hospital ten days after the MR scan. A powerful HD camera was used to record the operation for the validation.
Results & Discussion
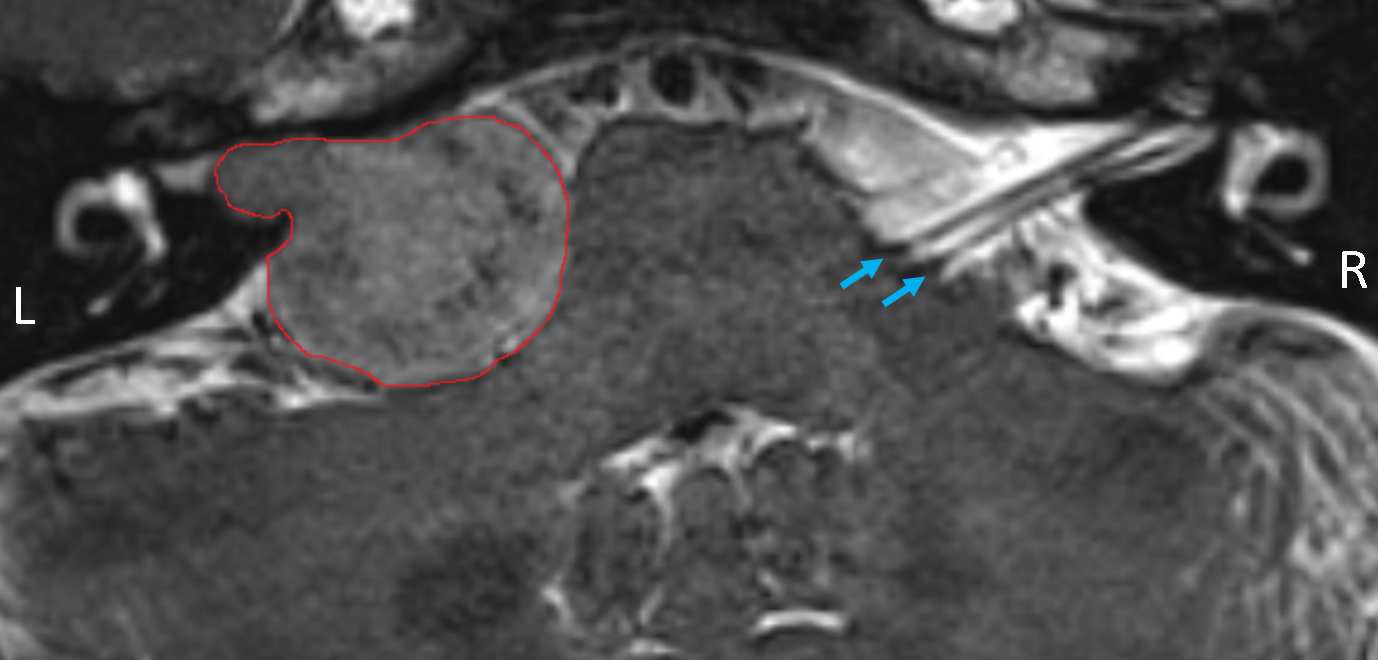
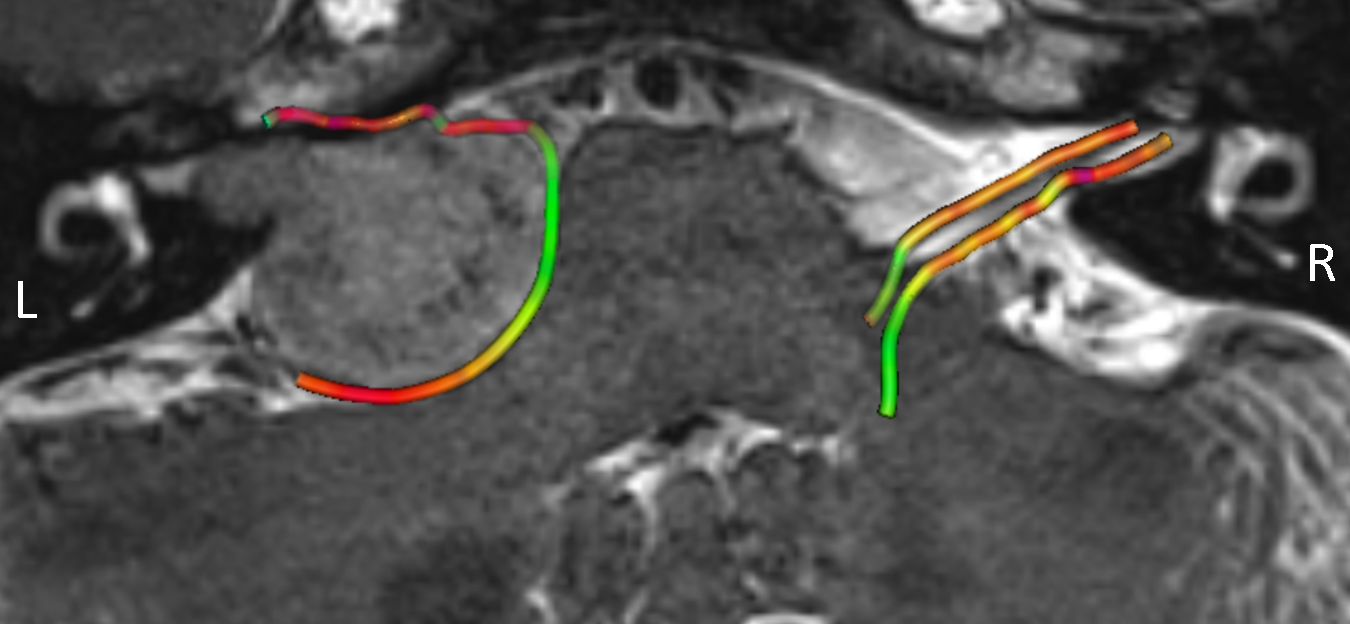
The facial nerve tractography in two patients has been studied, the figures here shows the result of one patient. In the anatomical T2 images of the patient shown in Fig.1, the vestibular schwannoma, observed on the left side brain, has invade the internal acoustic meatus and severely displaced the facial nerve, making it hard to determine the track. In contrast, on the normal (right) side of the brain, it is much easier to identify the facial nerve and vestibulocochlear nerve going through the cerebellopontine angle cistern to the internal acoustic meatus. The tractography of facial nerve on both sides was shown in Fig.2. The left facial nerve was displaced to the anterior of the schwannoma, and it appeared to be very close to the tumor boundary. On the other side, the normal facial nerve went smoothly into the brain directly.
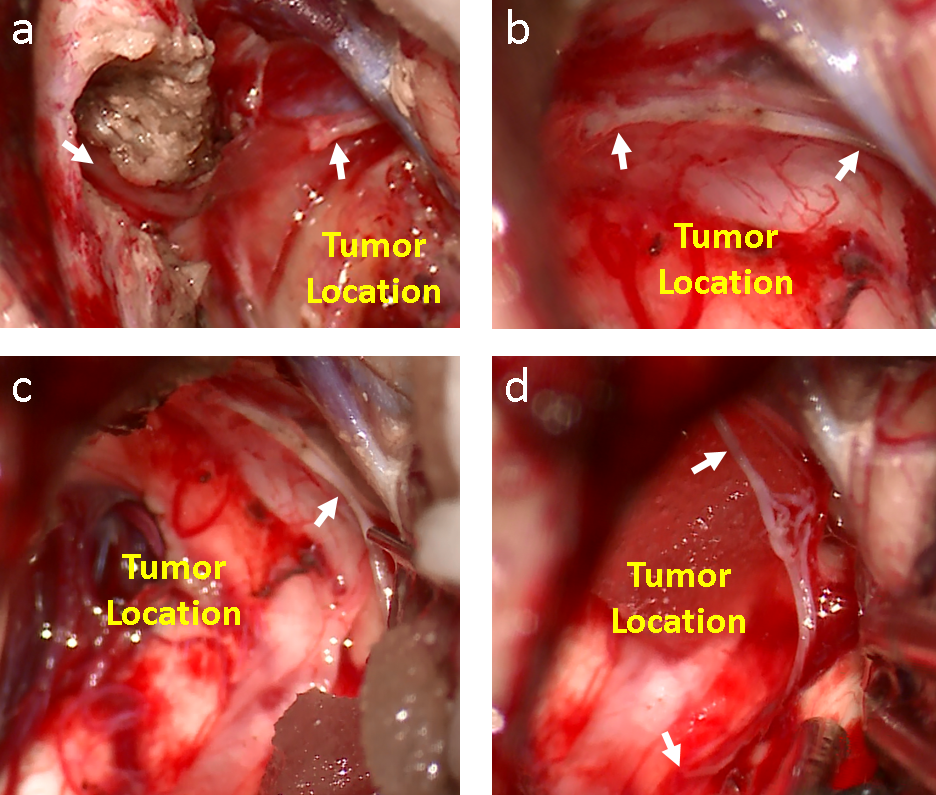
The actual location of the facial nerve was confirmed during the operation, as shown in Fig.3. The left facial nerve went out from the left internal acoustic meatus, and appeared to adhere to the anterior of the schwannoma, its pathway was just as the tractography shown. The surgeon scored the match between the tractography and observation in the operation and gave 5 (0 for not matched, and 5 for fully matched). In addition, during the operation, the facial nerve displaced by the schwannoma was observed to be stretched and became thinner than normal, indicating that the high resolution of diffusion acquisition is requisite for the tractography.
Conclusion
With the use of ZOOMit excitation for the anatomical images and RESOLVE for the diffusion images, it is possible to track the displaced facial nerve reliably and accurately, providing crucial information to the surgeons for making a better risk estimation and designing the surgical process before the operation.Acknowledgements
No acknowledgement found.References
1.Taoka T, Hirabayashi H, Nakagawa H, et al. Displacement of the facial nerve course by vestibular schwannoma: preoperative visualization using diffusion tensor tractography. Journal of Magnetic Resonance Imaging, 2006, 24(5): 1005-1010.
2.Gerganov V M, Giordano M, Samii M, et al. Diffusion tensor imaging-based fiber tracking for prediction of the position of the facial nerve in relation to large vestibular schwannomas: Clinical article. Journal of neurosurgery, 2011, 115(6): 1087-1093.
3.Roundy N, Delashaw J B, Cetas J S. Preoperative identification of the facial nerve in patients with large cerebellopontine angle tumors using high-density diffusion tensor imaging: Clinical article. Journal of neurosurgery, 2012, 116(4): 697-702.
4.Song F, Hou Y, Sun G, et al. In vivo visualization of the facial nerve in patients with acoustic neuroma using diffusion tensor imaging–based fiber tracking. Journal of neurosurgery, 2016: 1-8.
5.Hilly O, Chen J M, Birch J, et al. Diffusion Tensor Imaging Tractography of the Facial Nerve in Patients With Cerebellopontine Angle Tumors. Otology & Neurotology, 2016, 37(4): 388-393.
Figures