3473
Reducing complexity of functional imaging: free-breathing imaging based ADC and IVIM measurements are as accurate as breath-hold measurements in renal cell carcinoma1Department of Circulation and Medical Imaging, NTNU - Norwegian University of Science and Technology, Trondheim, Norway, 2Radiotherapy & Imaging, The Institute of Cancer Research, London, United Kingdom, 3Department of Radiology, The Royal Marsden Hospital, London, United Kingdom
Synopsis
Respiratory motion represents a serious confounding factor for abdominal imaging; for more complex diffusion models such as IVIM, acquisition of diffusion-weighted images in successive breath-holds offers control of motion for sharper images. In this patient study, DWI was performed in free-breathing and consecutive breath-holds, without registration, on successive days without intervention to determine repeatability. Derived tumour ROI parameters from ADC and IVIM models were not significantly affected between breathing regimes, but observed coefficients of variation for free-breathing were smaller for all pseudo-diffusion related parameters. Breath-holding is time inefficient, and free-breathing allows more data collection for development of robust DWI markers.
Introduction
The difficulty of imaging lesions in the abdomen is well known (1); substantial blurring arising from respiratory motion can severely compromise image quality, and confound interpretation and analysis of functional MR images. The increased use of longer, multiple-b-value diffusion-weighted imaging protocols such as Intravoxel Incoherent Motion (IVIM) suggest a demand for motion-compensating or control techniques at the point of acquisition, such as navigator-triggering or breath-hold. Post-processing techniques, most commonly registration, offer improvements to image appearance at the cost of off-line computational effort (2). In this study, patients with renal cell carcinoma underwent free-breathing (FB) and breath-holding (BH, in expiration) multiple-b-value DWI protocols on successive days, in order to assess the effect on derived diffusion parameter values and repeatability.Methods
Patients (n=11) with metastatic renal cell carcinoma gave informed consent, and underwent diffusion-weighted imaging with the following parameters: prototype single shot EPI, 3-scan-trace monopolar diffusion weighting, 5 mm slices acquired coronally (n=5) or axially (n=6), FOV 380x380 mm, resolution 1.5x1.5 mm in-plane (interpolated), iPAT factor 2, and with b-values 0, 20, 40, 60, 80, 100, 250, 500, and 750 mm-2s. For FB, NSA = 5 for a total acquisition time of 9 minutes; for BH, each 20 s breath-hold consisted of NSA = 1 for b = [0, X] where X is each successive non-zero b-value. Including resting time, the total time for BH acquisition was approximately 7 minutes. All images were used for analysis, conducted using in-house software (ADEPT, ICR, London UK) to fit both ADC and IVIM models, using a Markov Chain Monte Carlo approach on a voxel-by voxel basis within ROIs drawn around the tumour in 5 central imaging slices by an expert radiologist. Median values per ROI were recorded, and the results for each parameter tested for significance (p < 0.05) between successive days and breathing strategies using a multi-way ANOVA. Repeat-measures Coefficients of Variation (CoV) were calculated for each parameter and breathing strategy.Results
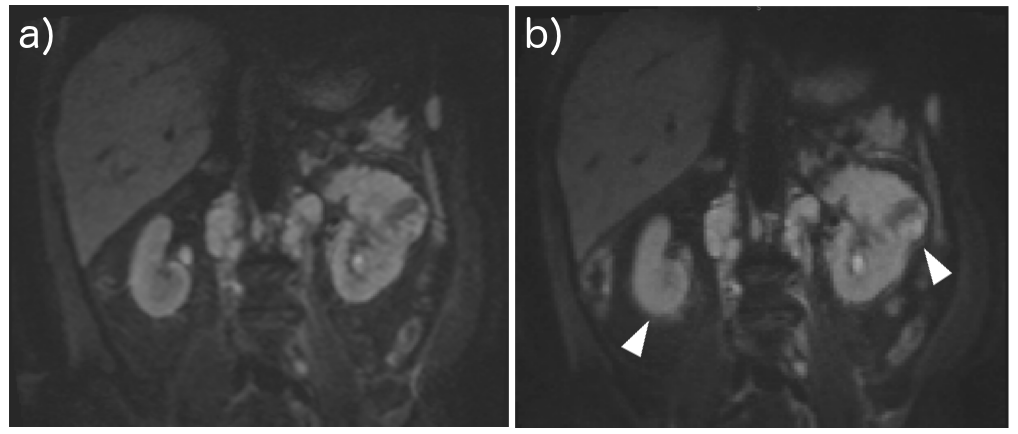
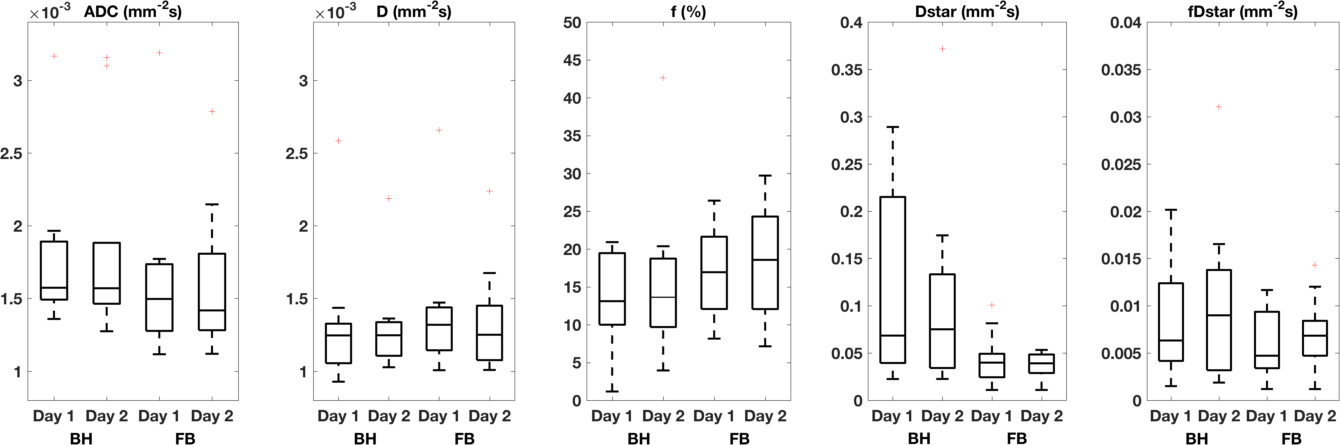
All FB data were acquired successfully on both days; data for BH were excluded for two patients on one visit owing to image artefacts, and so CoV calculations excluded these data. Lesions ranged in size from 30.5 to 1864.6 cm3, with CoV of voxel counts for BH and FB of 10.8 and 12.2% respectively. Images acquired in breath-hold appeared visually to suffer less from respiration blurring (Figure 1). The values for DWI parameters (median in ROI) are given in Table 1 as cohort mean ± s.d., and show good repeatability for ADC and D in both breathing regimes, with CoV values lower than 7%. The IVIM parameters associated with pseudodiffusion, f, D*, and the compound parameter fD*, have higher CoV values indicating lower repeatability, although in all cases these are smaller for FB compared to BH. The comparison of all parameters is shown in Figure 2; no significant difference was observed between BH and FB or between successive day’s scans for any of the parameter values (p = 0.19 and p = 0.40 respectively, ANOVA). The values for D were significantly lower than those for ADC for the corresponding day and breathing regime (p < 0.01, ANOVA), indicating the influence of observed non-monoexponential decay when using the ADC model, which implicitly assumes monoexponential behaviour.Discussion
The use of DWI parameters in lesion detection and characterisation relies both on their sensitivity and their robustness, and so acceptable repeatability is essential for critical assessment and interpretation of results. The desire to reduce blurring in diffusion images is borne of a visual frame of reference, but this contrasts with functional imaging studies that typically involve post-processing and analysis at an ROI level. In such cases, strategies to ameliorate respiratory motion may lead to increased patient discomfort, while the reduced efficiency of data acquisition compared to free-breathing does not benefit the accuracy or precision of resulting parameters, similarly to navigator-triggered acquisitions (3). Acquisition of successive breath-holds with a matched contrast (b=0) image may offer advantages for registration techniques, which may circumvent the difficulty of co-registering images with altered contrast; this introduces a considerable offline component to the data analysis, and will be explored in future work. In this study, parameters derived from a multiple-b-value abdominal DWI protocol in a patient cohort show no benefit of breath-holding over free-breathing for ADC and IVIM summary statistics in renal cell carcinoma; where robustness of analysis is improved by amount of sampling, the scanning efficiency of free-breathing improves the repeatability and thus performance of the resulting parameters for use as clinical biomarkers.Acknowledgements
CRUK and EPSRC support to the Cancer Imaging Centre at The Institute of Cancer Research and The Royal Marsden Hospital in association with the MRC and Department of Health (England) (C1060/A10334, C1060/A16464) and NHS funding to the NIHR Biomedical Research Centre and the Clinical Research Facility in Imaging at The Royal Marsden and the ICR. We acknowledge support from Siemens for use of work-in-progress DWI sequences.References
1. Koh D-M, Collins DJ, Orton MR. Intravoxel incoherent motion in body diffusion-weighted MRI: reality and challenges. Am J Roentgenol. 2011; 196(6):1351–61.
2. Guyader J-M, Bernardin L, Douglas NHM, Poot DHJ, Niessen WJ, Klein S. Influence of image registration on apparent diffusion coefficient images computed from free-breathing diffusion MR images of the abdomen. J Magn Reson Imaging. 2015; 42(2) 315-30.
3. Jerome NP, Orton MR, D’Arcy JA, Collins DJ, Koh D-M, Leach MO. Comparison of free-breathing with navigator-controlled acquisition regimes in abdominal diffusion-weighted magnetic resonance images: Effect on ADC and IVIM statistics. J Magn Reson Imaging. 2014; 39:235–40.
Figures